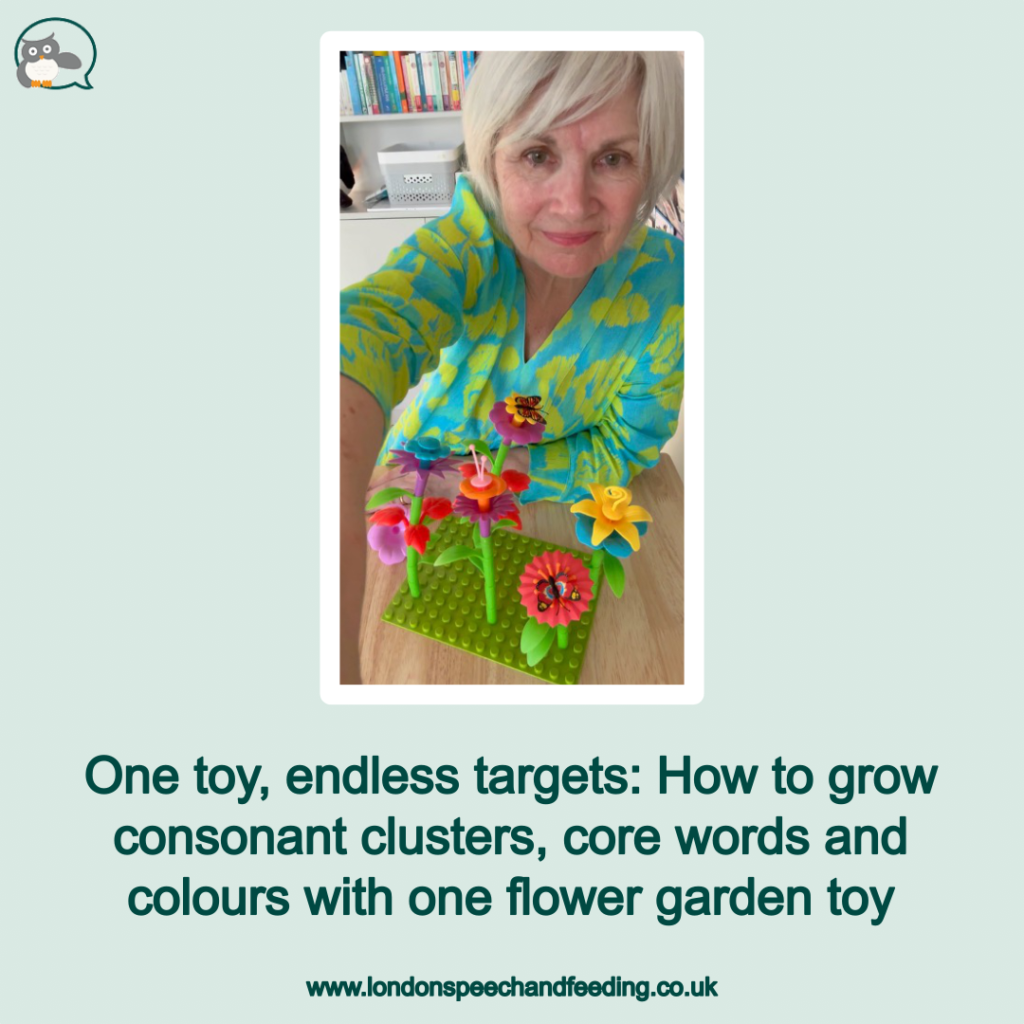
One toy, endless targets: How to grow consonant clusters, core words and colours with one flower garden toy

If you’ve been following me for a while you already know my absolute favourite rule for speech therapy: let the toy work for you. You don’t need an entire cabinet full of different flashcards or games to target a massive range of speech goals (though truth be told I do have 4 cabinets! What am I saying…) but often I find that sticking to one highly engaging, open-ended toy reduces a child’s cognitive load, keeps them firmly planted in play, and gives you dozens of natural opportunities for high-repetition practice. It also reduced my cognitive load!
In today’s post we are looking at a classic: The build-a-flower garden toy. A link is here: https://www.amazon.co.uk/Fivejoy-Flower-Garden-Building.
This vibrant, stacking toy isn’t just great for fine motor skills. It is an absolute goldmine for speech therapy. While it is incredible for targeting tricky consonant clusters (blends) like /ST/, /SP/, /SPR/, /FL/, /BL/, and /GR/, it is equally powerful for building functional core vocabulary.
1. Digging deep with /ST/
Let’s start building our garden.
Stem & stalk: ‘Look at this long stem!’ or ‘Can you put the stem in?’ or ‘do you want the green or the red stem’?
- Stuck: If a piece is a little tight to push down, it’s a brilliant opportunity for a natural exclamation: ‘Oh no, it’s stuck! Help me!’
- Stand: Once it’s secure, you can celebrate: ‘it can stand up now!’
- 👉 Core word integration: Use this setup stage to practise ANOTHER ONE. As you hold the base pieces, wait for the child to use their words or AAC device to request, ‘I want another one!’ before handing over the next stem.
2. Sowing seeds with /SP/ and /SPR/
Every good gardener needs the right equipment and a close eye for detail. We can introduce tools and descriptive language to hit our /SP/ and triple-blend /SPR/ targets.
- Spade: Grab a toy shovel or pretend to use one. ‘Let’s dig a hole with the spade.’
- Spot: Point to the holes on the base. ‘Find a good spot for this flower.’
- Sprout: Talk about the little green pieces: ‘Look at the little sprout!’
- 👉 Core word integration: Build on spontaneous requesting here. If they are eyeing a specific piece, model a full phrase like: ‘I WANT THE PINK ONE.’
3. /FL/ and fine motor actions
Now, we can start adding the colourful petals.
- Flower: This is your high-frequency word for the entire activity. ‘Put the green/blue/pink flower on top.’
- Flat & flutter: ‘This piece is flat on the ground,’ or ‘The butterfly flutters by!’
- 👉 Core word integration: This stage is perfect for teaching directional actions. Every time they stack a petal onto a stem, model the core phrase: ‘PUT IT ON!’
4. Blending it all together with /BL/
Building a garden is a fantastic sensory experience because of the vivid colours. We can lean heavily into the /BL/ sound by focusing on colour selection and the action of growth.
- Blue & bloom: ‘Should we use a blue flower?’ and ‘Watch it bloom!’
- Blade & blend: Point out the blades of grass and talk about how we blend all the colours together.
- 👉 Core word integration: Don’t just focus on putting the toy together, taking it apart is half the fun! If a child places a piece they don’t want, or when it’s time to clean up, model: ‘TAKE IT OFF.’
5. Working the /GR/
Finally, we look at the environment supporting our garden. The /GR/ blend can be targeted by looking downward at the base of our toy setup.
- Green: Nearly every stem and base piece in this toy is a vibrant shade of green.
- Grass & ground: ‘Put the base down on the ground.’ ‘Look at the green grass.’
- 👉 Core word integration: Combine your /GR/ blend with a powerful core phrase. As you pull a stem upward slowly or stack the petals higher and higher, chant together: ‘MAKE IT GROW! Grow, grow, grow!’
Maximise your repetitions in play
The beauty of the flower garden toy is its repetitive nature. Because a child builds multiple flowers, you aren’t just saying a word or a phrase once, you have the potential to repeat it 10, 15, or 20 times in a single sitting without the child losing interest.
By layering structural speech sounds (like blends) over functional communication phrases (like core words), we give children words they can use across their entire day.
What toy would you like to see us target next in our series? Let me know in the comments on Instagram, and don’t forget to swipe through the carousel there to save these word lists for your next playtime!
If you are concerned about your child’s speech, please do not hesitate to get in touch. I would love to help you find some answers.

Sonja McGeachie
Highly Specialist Speech and Language Therapist
Owner of The London Speech and Feeding Practice.



Find a speech and language therapist for your child in London. Are you concerned about your child’s speech, feeding or communication skills and don’t know where to turn? Please contact me and we can discuss how I can help you or visit my services page.