Getting down on their level: Why face-to-face play is a speech therapy superpower

As parents, we spend a massive portion of our days multi-tasking. We are talking to our toddlers while washing dishes, shouting encouraging words from across the living room while folding laundry, or answering their questions from a few feet above them while walking through the supermarket. It is a completely natural dynamic, after all, the adult world happens up here, and their world happens down there.
But when it comes to actively boosting your child’s speech and language development, one of the simplest, most profound changes you can make costs absolutely nothing and requires no special training.
It is simply this: Get down on the floor, sit cross-legged, and get face-to-face.
At London Speech and Feeding I call this physical positioning ‘face to face’. It is also one of the major ‘Hanen Programme’ Strategies. It completely reshapes how your child interacts with you, transforms how they process language, and turns ordinary playtime into an instant communication opportunity.
Our mouth is the magic: Visual cueing and speech imitation
When a child is learning to talk, they aren’t just listening to the sounds you make; they are watching how you make them.
Speech is an incredibly complex motor skill. To say a single word, the brain must coordinate the lips, tongue, teeth, jaw, and vocal cords in a fraction of a second. When you speak to your child from a standing or even a seated chair position while they are on the floor, your mouth is entirely out of their direct line of sight. They miss the visual roadmap of speech.
When you sit right in front of them at eye level:
- They see mouth shapes: They can see how your lips round for an /OO/ sound, how your teeth touch your lip for an /F/ sound, or how wide your mouth opens for an /AH/.
- They read facial expressions: Emotions give context to words. Seeing your eyes widen with excitement or your eyebrows lift in surprise helps them map meaning onto the vocabulary you are using.
- They mimic naturally: By putting your face directly in your child’s field of vision, you make it infinitely easier for her or him to try and copy your oral movements.
If you are working on a specific word like ‘pop’ while blowing bubbles or ‘more’ during snack time getting your face just a foot or two away from your child gives her or him the front-row seat she or he needs to learn the mechanics of that word.
Unlocking joint attention: The foundation of all languages
Before a child can say their first words, they need to master a milestone called joint attention.
What is joint attention?
It is the magic moment when a child looks at an object (like a toy train), looks up at you to share their excitement, and then looks back at the object. It is a three-way loop of shared experience.
Without joint attention, communication cannot thrive. If a child is entirely hyper-focused on a toy and ignoring your presence, or if you are commenting on a book they aren’t looking at, true communication isn’t happening.
When you get down on the floor on a play mat, you naturally insert yourself into their bubble. You aren’t a distant narrator anymore; you are a co-player. Being at their level makes it incredibly easy for their eyes to flick from the toy straight to your face. This shared gaze is the exact moment language takes root. It signals to the child, ‘We are experiencing this together, and this thing we are doing has a name.’
The ‘wait and see’ technique
Once you are down on the floor, the temptation is often to take over by pointing at everything, asking a million questions like ‘What’s that?’, ‘Is that a blue train?’, or somehow driving the play.
Instead, the most powerful thing you can do at eye level is to practise the ‘Wait and See’ technique.
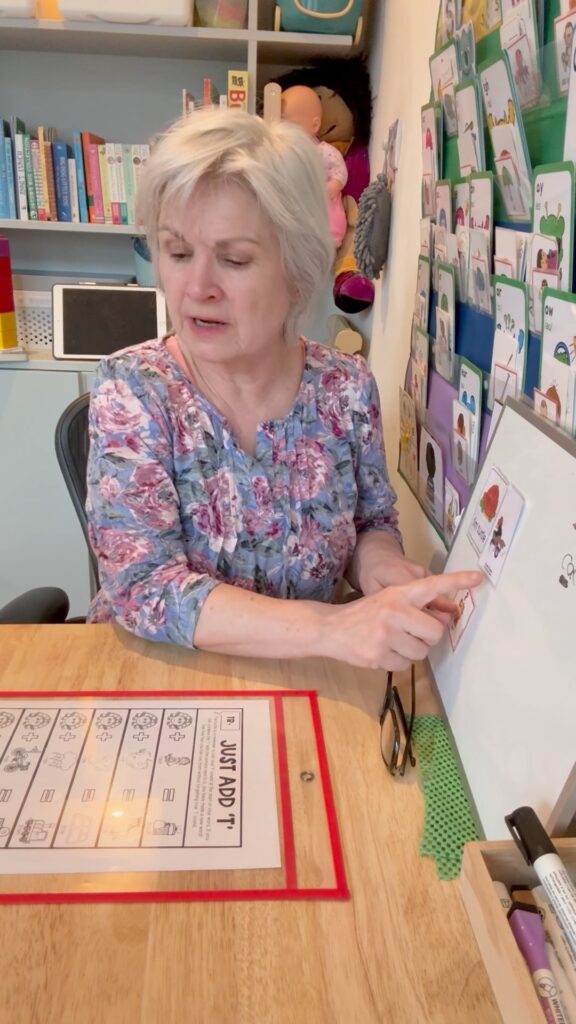
In the video clip you can see this exact dynamic in action. Look at how I am sitting cross-legged on the mat, at eye level with the toddler. Notice how my hands are on the toy container, but my eyes are locked on the child. I am not forcing the interaction; instead, I am waiting.
Here is how you can use this strategy at home:
- Set the stage: Get down on their level with a high-interest toy that requires help (like a wind-up toy, bubbles, or a tight-lidded box with toys inside).
- Create anticipation: Hold the object near your face or place your hands on it, but don’t open or activate it right away.
- Lean in and wait: Lean slightly forward, open your eyes wide, adopt an expectant facial expression, and completely pause. Count to five or ten in your head. Do not say anything.
- Capture the gaze: Wait for the exact moment your child looks up from the toy to meet your eyes, as if to say, ‘Well? Are you going to open it?’
- Reward the eye contact: The instant they make eye contact, deliver the language reward! Model a simple, functional word like ‘Open!’, ‘Go!’, or ‘Look!’ as you immediately do the action.
By pausing and waiting at eye level, you create a ‘communication temptation’. The child learns that looking at you and engaging with your face is the key that unlocks the fun.
Making it a daily habit
You don’t need to spend hours a day sitting on the floor to see a difference. Start small by dedicating just 10 to 15 minutes of undivided, face-to-face play time each day. Turn off the television, put your phone in another room, get down on their level, and let them lead the play while you focus on being their visual communication partner.
Whether you’re opening a little toy briefcase, pushing a plastic train along a track, or stacking blocks, remember: your face is the best toy in the room.
Are you wondering if your toddler’s speech and language milestones are on track? At London Speech and Feeding I love helping families navigate early communication. Feel free to explore my services page and reach out directly to schedule a consultation.

Sonja McGeachie
Highly Specialist Speech and Language Therapist
Owner of The London Speech and Feeding Practice.



Find a speech and language therapist for your child in London. Are you concerned about your child’s speech, feeding or communication skills and don’t know where to turn? Please contact me and we can discuss how I can help you or visit my services page.