
Ten games to support communication in primary school aged children
When parents visit me with their child, their stress is palpable. Often parents don’t relish or even expect to be asked to practise strategies at home with their child between sessions. Let alone to practise whilst on holiday. I understand that you don’t necessarily want anything extra added to your daily ‘to do’ lists. This is why we try our best to incorporate all speech and language therapy practice into children’s daily activities.
For example:
- during bath time;
- mealtimes;
- getting ready for bedtime;
- story time
- yes, playtime!
These are activities that all parents will engage with anyway, so it seems to make sense to incorporate both. This is to avoid adding extra pressure on parents’ already stressful and time-poor daily lives. I am hoping my blog will come in handy, especially for the summer holidays.
On holiday you are unlikely to have your usual games and toys with you – so here is a nice little list of things you can use instead of traditional games and toys:
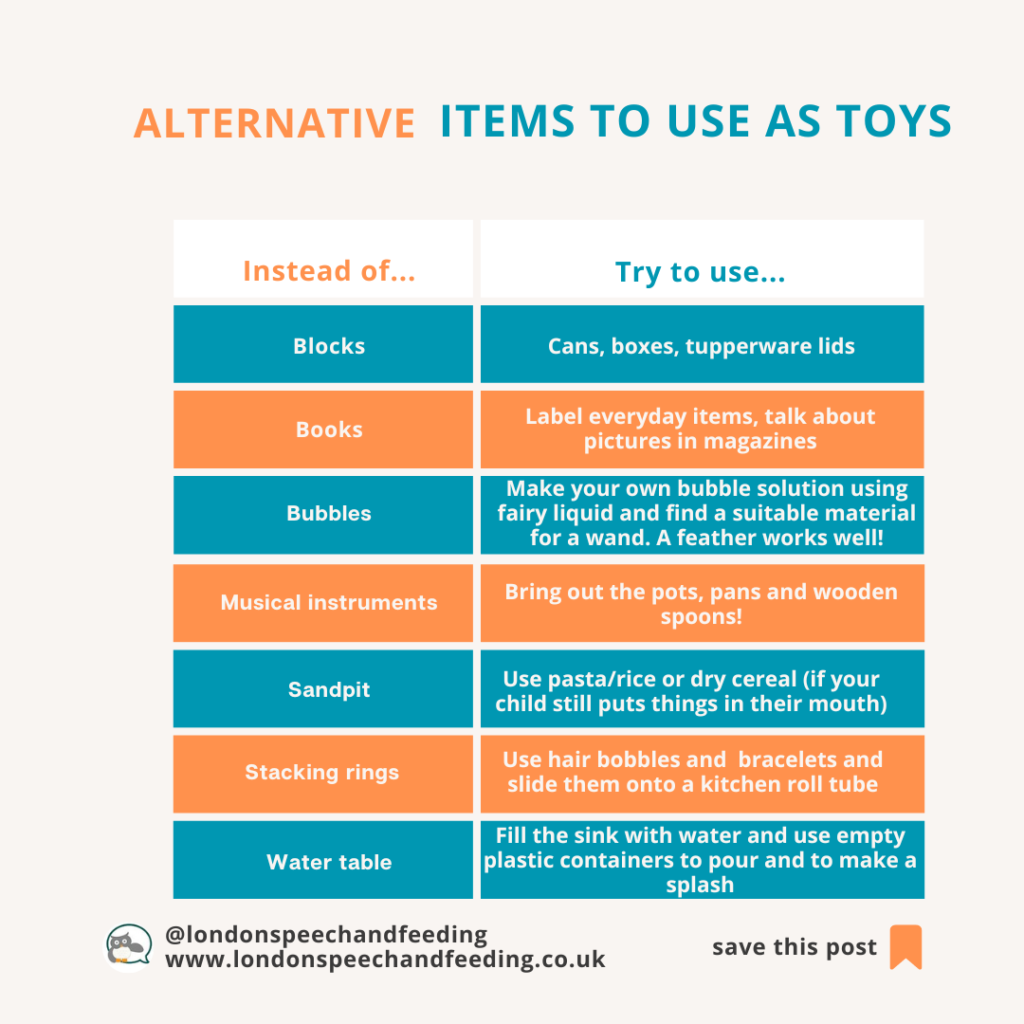
If you can think of any other alternatives on holiday and would like to tell me about them, I would love to see your comments below. We can never have too many holiday games!!
If you are at home over the summer and you do have some games in the cupboard you might want to dust these ones down or buy one or two new ones (if you want to).
Most games have multiple uses, and it’s always best to adapt a game to match your child’s interests and what motivates them.
So let’s start…
- Pop up pirate: pop a sword into the barrel and watch the pirate pop up randomly. Practise social skills, speech sounds, expressive language (e.g., put a sword on a picture, say the word/sentence then pick up the sword and push it into the barrel).
- Word games such as ‘ISpy’, ‘I went to the shop and I bought…’, ‘describe a person and guess who they are’: perfect for when you’re on the move, whether travelling or walking. You can play this anywhere and still support speech, language and communication. You could play ISpy using your child’s special sound, or ‘I went to the shop and bought all things beginning with [insert special sound here]’.
- Shopping list: Orchard game is a game to practise categorising. We explain the analogy of the brain being like a filing cabinet. If information is all in the correct place, it’s easier to find, retrieve and use. You can also practise specific speech sounds in this activity. You could also put the words in a sentence to add more of an expressive language element.
- Wiggly worms: this Orchard game is all about phonological (awareness of sounds) awareness. Matching a letter with the word. You can also practise the sounds in the words (e.g, g-o-l-d = gold; m-a-ke = make). Talk about the elements, e.g., ‘g-o-l-d’ has 4 sounds, 1 syllable; ‘m-a-ke has 3 sounds, one syllable. You can talk about what words rhyme with the different words and what makes a rhyming word (i.e., the middle and end sounds remain the same).
- Sound detectives: this Orchard game allows children to identify sounds. It also has an app (if your child prefers a tech-way of learning). Children identify the sound then they can add the picture card to their path and become closer to being a successful detective. This game can also support memory skills.
- Conversation cubes: throw the dice and start building a story. You can also create and use ‘colourful semantics’ sentence strips to support expressive (spoken) language as support to build the narrative.
- Think words: ‘name it, press it, pass it’. A great game to expand word knowledge. You can talk about the words at the end of each round exploring semantic (meanings) and phonemic (sounds) links. Your child can also develop social skills (such as attention, listening and turn-taking).
- Poo bingo: this is perfectly disgusting but equally fun for kids of about 3.5 years plus – if your child’s target is to practise /p/ sound this is the one for you. You can also learn all about the different animal’s poo, which I am sure you have always wanted to do!! The more we know about a word, the easier it is to store, retrieve and use. Yes, even talking about poo can help!! Also, it’s great for our visual learners.
- Simon says: a game that can be played indoors or outdoors. Parents can take turns being “Simon” and give various commands that your child must follow. This means that your child can practise their receptive (understanding of) language as well as their expressive language, speech sounds and social skills (such as turn-taking and initiating).
- Ker-plunk: this is perfect for practising your child’s special sound. Repetition is very important, but also can be monotonous, so finding a game that they enjoy is vital. Take turns to pull out a stick. Next, your child can either say their special sound or word (depending on what stage they are at) or hear a good model from other players.
Do you still have questions? Contact Sonja for support.
Find a speech and language therapist for your child in London. Are you concerned about your child’s speech, feeding or communication skills and don’t know where to turn? Please contact me and we can discuss how I can help you or visit my services page.














