If your child is using echolalia and/or has a diagnosis of autism, then your child’s way of processing language is most likely different to the classic way children typically learn language. We call this process Natural Language Acquisition or Gestalt Language Processing.
Step by Step guide to Gestalt Learning
Let’s explore the following stages of Gestalt Processing:
Stage 1: communicative use of whole language gestalts
(e.g., “let’s get out of here”)
Children and young people in this stage use echolalia. They need to hear more gestalts or scripts. So, your job is to model, model, model and to use functional language that your child can repeat back.
Stage 2: mitigated into chunks and re-combining these chunks
(e.g., “let’s get” + “some more”) and (e.g., “let’s get” + “out of here”)
This is when you take parts of gestalts or phrases and then combine it with other parts.
Stage 3: further mitigation (single words recombining words, formulating two-word phrases)
(e.g., “get…more”)
They are going beyond their gestalts. Furthermore, they may begin to label different objects.
Stage 4: formulating first sentences
(e.g., “let’s get more toys”)
You may see more grammatical errors during this phase as they are creating unique sentences. Please don’t worry about this, it means they are playing and experimenting with language. As communication partners, you could model the correct form of the sentence.
Stages 5 & 6: formulating more complex sentences
(e.g., “how long do you want to play inside for?”)
You can see that language learning is a process, that is trialled and tested, used in different contexts for children to be able to learn and use language appropriately.
My next blog will give you activities ideas and how you might use them specifically with a Gestalt Language Processor.
Remember early intervention is vital. So, if you have any concerns, please seek the advice of a Speech and Language Therapist.
Find a speech and language therapist for your child in London. Are you concerned about your child’s speech, feeding or communication skills and don’t know where to turn? Please contact me and we can discuss how I can help you or visit my services page.
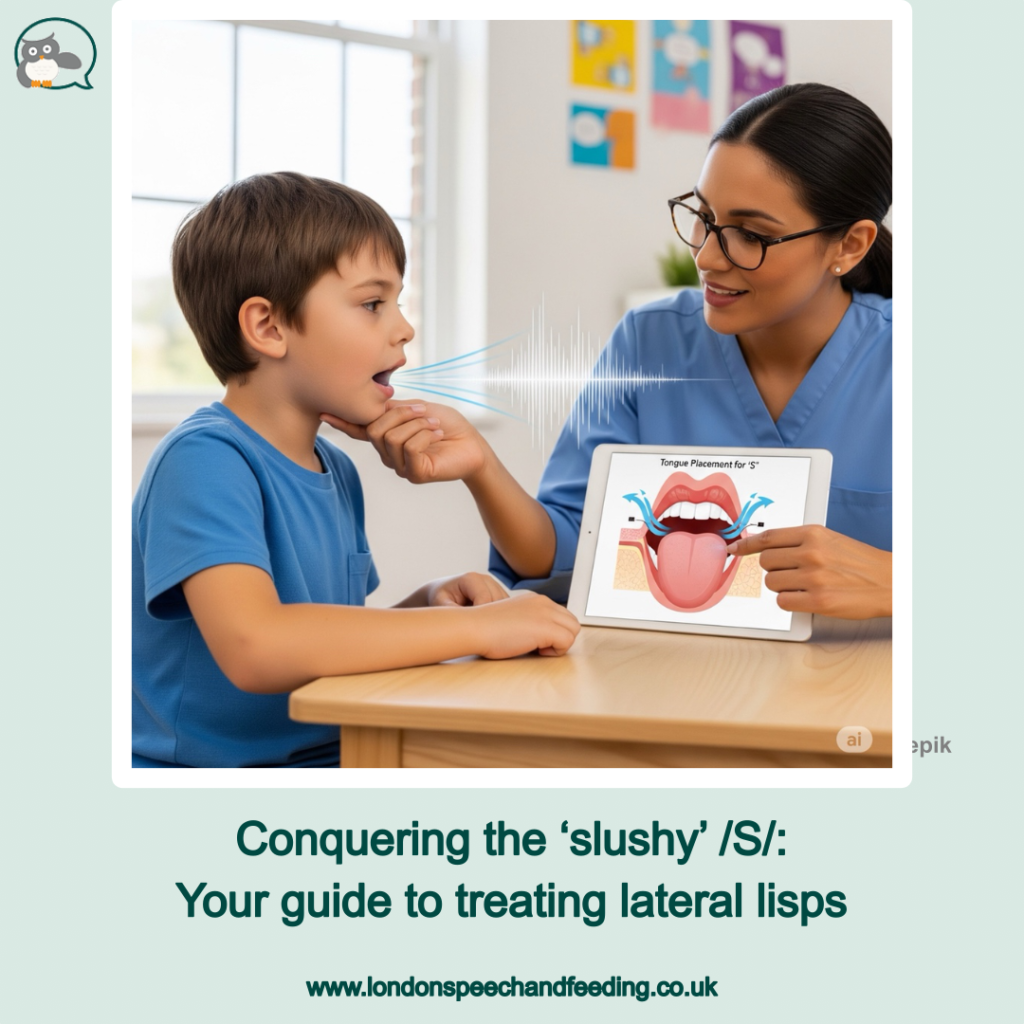
As a speech therapist, few things are as rewarding as helping a child find their clear, confident voice. Among the various speech sound disorders, the ‘lateral lisp’ – often described as a ‘slushy’ or ‘wet’ /S/ sound – presents a unique challenge. While it can be tricky to treat, I’m thrilled to share that I’ve had significant success in helping children overcome this particular hurdle.
What is a lateral lisp?
Most people are familiar with a frontal lisp, where the tongue protrudes between the front teeth, resulting in a /TH/ sound for an /S/ (e.g., ‘thun’ for ‘sun’). A lateral lisp, however, is different. Instead of the air escaping over the front of the tongue, it escapes over the sides, often giving the /S/ and /Z/ sounds a distinct, muffled, or ‘slushy’ quality. This happens because the tongue is not forming the correct central groove, allowing air to spill out laterally.
The science behind a perfect /S/ vs. a slushy one
To understand how to fix a lateral lisp, it’s helpful to understand how a ‘perfect’ /S/ sound is made. Imagine a narrow, focused stream of air. For a clear /S/ sound, your tongue forms a shallow groove down its centre, directing a precise, thin stream of air right down the middle, over the tip of your tongue, and out through a tiny opening between your tongue and the roof of your mouth, just behind your front teeth. This focused airflow creates that crisp, sharp /SSSS/ sound we recognise.
Now, picture what happens with a lateral lisp. Instead of that neat, central channel, the tongue is often flatter or positioned in a way that allows the air to escape over one or both sides. Think of it like a river overflowing its banks – the air, instead of flowing in a controlled stream, spills out sideways, creating that characteristic ‘slushy’ sound. This lateral airflow is what we need to retrain.
Why is it tricky to treat?
Treating a lateral lisp can be challenging for a few reasons:
Habitual muscle memory: The way the tongue moves and positions itself for a lateral lisp is deeply ingrained. It’s a motor habit that needs to be unlearned and replaced with a new, more precise movement.
Subtle differences: The difference between a lateral lisp and a correct /S/ sound can be quite subtle to perceive, both for the child and sometimes even for parents. This makes it harder for the child to self-monitor and correct.
Oral motor control: It requires fine motor control of the tongue muscles to create and maintain that central groove for airflow.
My success with children aged six years and over
I’ve found great success in treating lateral lisps, particularly with children aged six years and older. Why this age group? By this age, children typically have:
Increased awareness: They are more aware of their speech and often more motivated to make changes. They can better perceive the difference between their ‘slushy’ /S/ and a clear one.
Improved cognitive skills: They can understand and follow more complex instructions and strategies.
Better self-monitoring: Their ability to listen to themselves and correct their own speech improves significantly.
Enhanced oral motor control: Their fine motor skills, including those of the tongue, are more developed, allowing for greater precision.
My approach focuses on a combination of auditory discrimination, tactile cues, and targeted myofunctional exercises to help children ‘feel’ the correct airflow and tongue placement. We use a variety of engaging activities to make the process fun and effective.
It is crucial to understand tongue functioning and focusing on correcting improper oral resting posture and muscle function, which are often significant contributors to a lateral lisp. For example, if the tongue rests low and wide in the mouth consistently, or if there’s a tongue thrust during swallowing, these habits can prevent the tongue from achieving the precise, midline placement necessary for a clear /S/ or /Z/ sound. Through targeted exercises I aim to re-educate the oral and facial muscles, promoting correct tongue posture at rest, during swallowing, and, ultimately, during speech production. By strengthening the muscles responsible for tongue lifting and encouraging a more appropriate swallowing pattern we can establish the correct oral motor skills needed to overcome a lateral lisp and achieve clearer articulation.
The recipe for success: Little and often
The single most crucial ingredient for success in treating a lateral lisp is daily home practice of all the strategies given. This isn’t about long, arduous sessions; it’s about consistency. Think of it like building a muscle: short, frequent workouts yield better results than sporadic, intense ones.
My recommended formula is ‘little and often’. This means:
Short, focused sessions: Aim for 5-10 minutes of practice, 2-3 times a day. This prevents fatigue and keeps the child engaged.
Integrate into daily routines: Practise while waiting for dinner, during a car ride, or before bedtime. Make it a natural part of their day.
Positive reinforcement: Celebrate every small success! Encouragement goes a long way in building confidence and motivation.
Parental involvement: Parents play a vital role in providing consistent cues and encouragement at home. I equip families with clear, easy-to-follow strategies.
Overcoming a lateral lisp requires dedication, but with the right guidance and consistent practice, a clear, confident /S/ sound is achievable. If your child is struggling with a ‘slushy’ /S/, please don’t hesitate to reach out. Together, we can achieve success!
Sonja McGeachie
Highly Specialist Speech and Language Therapist
Owner of The London Speech and Feeding Practice.
Find a speech and language therapist for your child in London. Are you concerned about your child’s speech, feeding or communication skills and don’t know where to turn? Please contact me and we can discuss how I can help you or visit my services page.
Does your child struggle to focus on toys or activities? Do they dart away as soon as you approach? You’re not alone!
The key to unlocking your child’s potential lies in following their lead. Let them guide the play session, and watch their engagement and focus soar.
Why Child-Led Play Works:
Empowerment: Children feel in control, sparking their curiosity and motivation.
Focused attention: They’ll stay engaged with activities for longer periods.
Reduced frustration: By stepping back and observing, you eliminate the pressure and stress that often comes with directed play.
How to Implement Child-Led Play:
Prepare the environment: Set out a limited selection of engaging toys.
Observe and wait: Sit back, watch, and listen to your child’s interests.
Embrace the moment: Resist the urge to direct or question; simply enjoy the process.
Remember: This simple approach can transform playtime and support your child’s development. Give it a try for a week and see the difference!
#OWLing #hanenmorethanwords
Observe, Wait, Listen. It’s a powerful formula for unlocking your child’s potential.
You will likely see:
Your child will stay put with any toy for longer whilst you are near them.
Your child will tolerate you being nearby and he/she won’t move away.
Your child will start giving you brief glances of enjoyment, or perhaps they will hand things to you, or they might take your hand and lead it to something that needs opening etc.
In other words, you will see that there suddenly is JOINT PLAY. Yes, granted it may not be according to your adult agenda, but there will be more togetherness than there was before. And this is the START of communication and social engagement.
USE Core words and a coreboard — to help your child understand the power of words
Core words are the building blocks of communication. Try using a coreboard like the one below, they are versatile and can be used in countless ways. By modelling these words naturally during play, you expose your child to their meaning and function in context. This approach is far more effective than isolated drill and practice, more powerful than flashcards!
Combining child-led play and AAC modelling creates a magic effect. To summarise:
Increased engagement: When you follow your child’s lead, they are more likely to be engaged and receptive to learning. This creates optimal conditions for introducing AAC core words.
Natural learning: By modelling AAC core words in the context of play, you help your child understand their meaning and purpose naturally. This fosters generalisation and spontaneous use.
Building relationships: Shared play experiences strengthen the bond between you and your child. This trust and connection are essential for successful communication.
Reduced pressure: Modelling AAC core words without expectation removes the pressure to produce language. This allows your child to explore communication at their own pace.
Expanded vocabulary: As your child becomes more comfortable with AAC, they will begin to incorporate core words into their own communication. This leads to vocabulary growth and increased independence.
Practical Tips
Observe and respond: Pay close attention to your child’s interests and actions. Respond to their cues with enthusiasm and support.
Keep it simple: Start with a few core words and gradually introduce new ones as your child’s skills develop.
Be patient: Language learning takes time. Celebrate small successes and avoid frustration.
Have fun: Remember, play is supposed to be enjoyable for both you and your child. Relax and have fun together!
Let’s say your child is playing with a pop-up toy like you see me do in the above photograph. Here, I followed my child’s lead by waiting to see what she wanted to do with the toy. You are now OWLING! (Observe Wait and Listen)
Once I noticed that there was repetitive opening of the flaps going on I then pointed to OPEN and MORE on the board, as I said: ‘let’s OPEN this one’ / let’s see MORE animals’ / ‘MORE cow! it says moo!’ ‘OPEN another one’ and so on.
Important to know, we are not expecting our child to respond verbally or with AAC, but we are providing language input and demonstrating how these words can be used with enthusiasm.
Naturally in time your child will look at the board and at your pointing and they will eventually want to copy you!
By incorporating these strategies into your daily interactions, you can create a supportive environment that fosters language development and communication growth. If you would like more guidance please get in touch and book in for a consultation, some individual therapy and/ or some parent coaching.
I look forward to supporting you. Please contact me and let’s see how.
Sonja McGeachie
Early Intervention Speech and Language Therapist
Feeding and Dysphagia (Swallowing) Specialist The London Speech and Feeding Practice
The London Speech and Feeding Practice
Find a speech and language therapist for your child in London. Are you concerned about your child’s speech, feeding or communication skills and don’t know where to turn? Please contact me and we can discuss how I can help you or visit my services page.
A Day In The Life Of An Independent Speech And Language Therapist
I often get asked how many clients/children I see per working day or what my working day/life looks like. I always reply that every day is different, which is true, but there is a sort of average working day which looks a bit like this:
I usually start preparing for my first client of the day at around 9.30 am: I clean the room, wipe down all the toys and materials (that’s if they are coming to my clinic room) and then it takes me about 30 minutes to select and sometimes make suitable materials, games and activities for the child’s therapy programme. Client arrives at 10.30 am and the fun begins. They leave around 11.30am, and the cleaning and wiping down starts again – yes it’s the pandemic but to be fair I would do this anyway. I quickly write up my notes and send home work to the client via email. Now it’s 12 noon and I start preparing for the next client at 12.30 pm. This might be online parent-child interaction coaching and so I need different materials and activities that are suitable for teletherapy. We finish around 1.30 pm and I will write up my notes before having some lunch.
Lunch tends to not be around 30 minutes. Around 2.00 pm I start prepping again for the next client: selecting activities, going over their last session, making sure I have everything I need to start at 2.45pm – we finish at 3.45pm, I write up my notes and then have a cuppa. The next client might be more on-line coaching or a child coming to see me: room cleaned and tidy, materials and activities prepared: client arrives at 4.30 pm and we finish at 5.30 pm. I clean the toys again, write up my notes and it is 6.00 pm ready for dinner. So that was four clients between 9 am and 6pm allowing for preparation, aftercare, cleaning and coffee and lunch.
Other days I might see three clients and do more admin like ordering toys or books or teletherapy activities, or making materials (we therapist make tons of materials, we’d put Blue Peter to shame!) Sometimes I do two home visits, one in the morning and one in the afternoon – the travelling/parking in London is so time consuming that it really reduces the number of clients I can see which is why I don’t do many of those.
I hand pick my clients to make sure that we are a good fit, and my service is bespoke: no one client gets the same treatment as another; each client is unique, usually very well-known and always highly valued. That takes time and means that in reality each client gets about 2 hours of my time, that is the actual session plus all the preparation and aftercare.
I love this way of working and would not ever want to return to seeing tons of clients each day, not knowing any of them really well, due to high caseload numbers, staff shortages and an overload of administration.
My way of working affords all my lovely clients the help they need to be able to feel empowered and to then support their children to make progress; when working with children they make the best progress they can make, fulfilling their potential. My lovely reviews and testimonials tell me that my clients appreciate the extra attention.
Find a speech and language therapist for your child in London. Are you concerned about your child’s speech, feeding or communication skills and don’t know where to turn? Please contact me and we can discuss how I can help you or visit my services page.
Communication is the essence of human interaction, allowing us to express thoughts, feelings, wants and needs. For non-speaking children and their families finding an avenue to communicate effectively can be a really challenging journey.
Augmentative and Alternative Communication (AAC) offers a solution: with AAC Core Boards as a powerful ally and tool to empower and express more than requests: ideas, comments, surprise and delight, as well as saying no to something! Very important!
“AAC is a set of tools and strategies that an individual uses to solve every day communicative challenges. Communication can take many forms such as: speech, a shared glance, text, gestures, facial expressions, touch, sign language, symbols, pictures, and speech-generating devices” (RCSLT, 2023) to name just some.
AAC Core Boards are a powerful tool to empower non-speakers to express ideas. In this blog, we’ll explore the significance of AAC Core Boards and how they can unlock the world of communication for non-speaking children.
Let’s discover and understand AAC Core Boards
Firstly, let’s look at what a Core Board looks like…
AAC Core Boards are a specific type of AAC system that employs a grid-style board. This grid contains a set of core vocabulary words or symbols, which serve as a foundation for all communicative functions (e.g., initiating, greeting, requesting, negating, commenting, asking a question, and expressing surprise).
These boards incorporate high-frequency (most used) and versatile words. They enable us to construct sentences, express emotions, and take part in conversations, fostering a sense of independence and autonomy. By enabling communication, we also remove some of the frustration (from not being able to communicate) which contributes/or often leads to behavioural difficulties.
Building literacy skills
AAC Core Boards are not only tools for immediate communication. They also play a pivotal role in language and literacy development. By using these boards, non-verbal children engage with words and symbols. It reinforces their understanding of language structure and grammar.
As they consistently play with and then use their boards, they naturally absorb language patterns, laying the foundation for improved literacy skills. This immersive learning experience paves the way for future language acquisition and communication growth.
Customisation for individual needs
Every child is unique, and their communication needs can vary significantly. AAC Core Boards are designed with this diversity in mind, allowing for customisation to suit individual preferences and abilities. The boards can be adapted to include specific vocabulary relevant to a child’s daily life, interests, and activities. This personalisation ensures that the AAC Core Board is a true reflection of your child’s personality and needs, making communication more motivating, engaging and effective.
Collaboration between AAC Core Boards and Speech Therapy
AAC Core Boards are an excellent tool but we need to know one important aspect: they only work well when used regularly by the child’s family and key people in the first place.
The board needs to be used and modelled by adults consistently and regularly across environments. This is so our children know what to expect, take an interest and begin to use the boards themselves. Modelling the use of AAC Core boards is vital. Think how long it typically takes for a child to learn their first word. Around a year! During that time the adults talk constantly to their child without hesitation or expectation! The same goes for introducing this new way of communicating.
Collaborating with your child’s Speech and Language Therapist (SLT) ensures that your child receives the right guidance in using the AAC system. SLTs can assess your child’s communication abilities, recommend appropriate boards and provide guidance on how to best put them in place, so that your child can reach their communicative potential.
For non-speaking children, AAC Core Boards are more than just tools. They are bridges to a world of communication, connection, and empowerment. These boards harness the power of visual communication, foster language development, social interaction, and personal expression. They can be tailored to individual needs with the support of skilled professionals. AAC Core Boards offer a beacon of hope, helping to break through communication barriers and thrive in a world that is waiting to hear your child’s voice.
For answers to your questions and to explore the most effective support for your child, feel free to contact us.
Find a speech and language therapist for your child in London. Are you concerned about your child’s speech, feeding or communication skills and don’t know where to turn? Please contact me and we can discuss how I can help you or visit my services page.
As parents, we spend a massive portion of our days multi-tasking. We are talking to our toddlers while washing dishes, shouting encouraging words from across the living room while folding laundry, or answering their questions from a few feet above them while walking through the supermarket. It is a completely natural dynamic, after all, the adult world happens up here, and their world happens down there.
But when it comes to actively boosting your child’s speech and language development, one of the simplest, most profound changes you can make costs absolutely nothing and requires no special training.
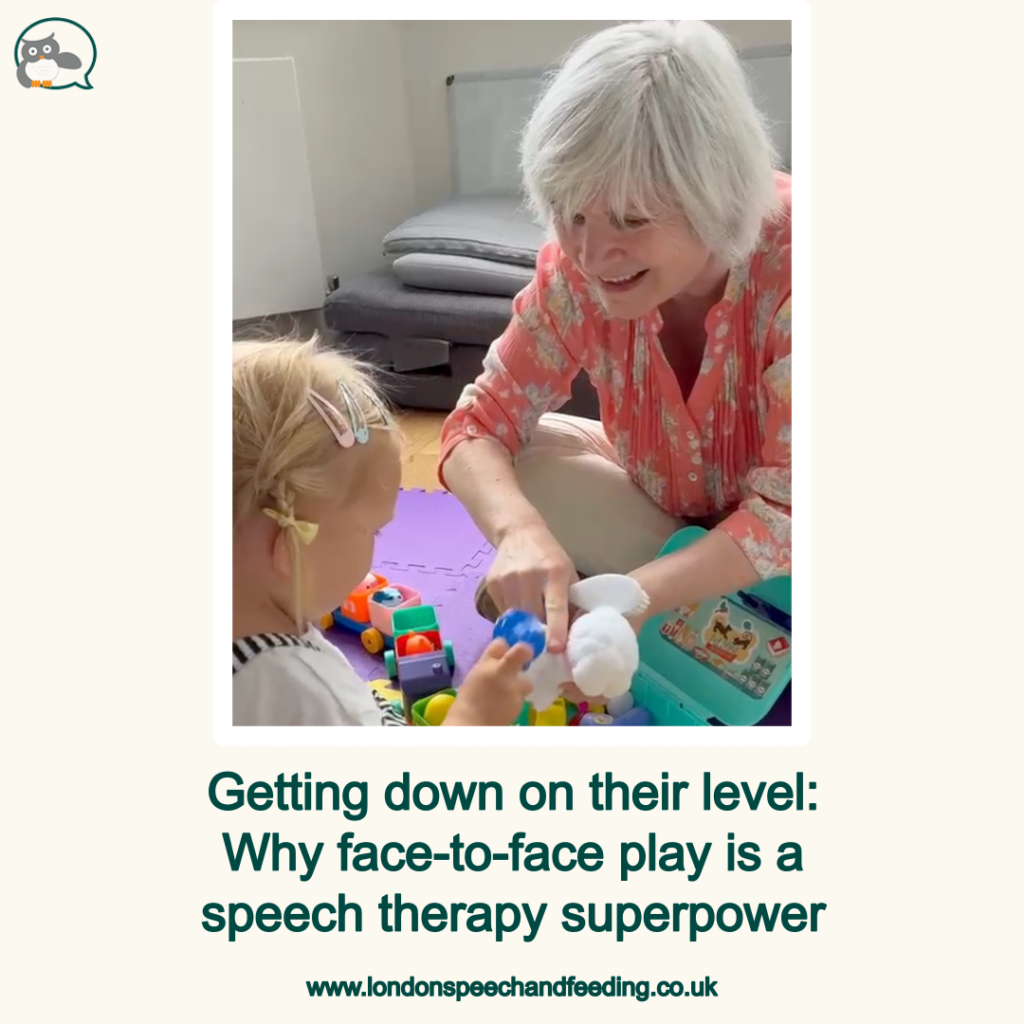
It is simply this: Get down on the floor, sit cross-legged, and get face-to-face.
At London Speech and Feeding I call this physical positioning ‘face to face’. It is also one of the major ‘Hanen Programme’ Strategies. It completely reshapes how your child interacts with you, transforms how they process language, and turns ordinary playtime into an instant communication opportunity.
Our mouth is the magic: Visual cueing and speech imitation
When a child is learning to talk, they aren’t just listening to the sounds you make; they are watching how you make them.
Speech is an incredibly complex motor skill. To say a single word, the brain must coordinate the lips, tongue, teeth, jaw, and vocal cords in a fraction of a second. When you speak to your child from a standing or even a seated chair position while they are on the floor, your mouth is entirely out of their direct line of sight. They miss the visual roadmap of speech.
When you sit right in front of them at eye level:
They see mouth shapes: They can see how your lips round for an /OO/ sound, how your teeth touch your lip for an /F/ sound, or how wide your mouth opens for an /AH/.
They read facial expressions: Emotions give context to words. Seeing your eyes widen with excitement or your eyebrows lift in surprise helps them map meaning onto the vocabulary you are using.
They mimic naturally: By putting your face directly in your child’s field of vision, you make it infinitely easier for her or him to try and copy your oral movements.
If you are working on a specific word like ‘pop’ while blowing bubbles or ‘more’ during snack time getting your face just a foot or two away from your child gives her or him the front-row seat she or he needs to learn the mechanics of that word.
Unlocking joint attention: The foundation of all languages
Before a child can say their first words, they need to master a milestone called joint attention.
What is joint attention?
It is the magic moment when a child looks at an object (like a toy train), looks up at you to share their excitement, and then looks back at the object. It is a three-way loop of shared experience.
Without joint attention, communication cannot thrive. If a child is entirely hyper-focused on a toy and ignoring your presence, or if you are commenting on a book they aren’t looking at, true communication isn’t happening.
When you get down on the floor on a play mat, you naturally insert yourself into their bubble. You aren’t a distant narrator anymore; you are a co-player. Being at their level makes it incredibly easy for their eyes to flick from the toy straight to your face. This shared gaze is the exact moment language takes root. It signals to the child, ‘We are experiencing this together, and this thing we are doing has a name.’
The ‘wait and see’ technique
Once you are down on the floor, the temptation is often to take over by pointing at everything, asking a million questions like ‘What’s that?’, ‘Is that a blue train?’, or somehow driving the play.
Instead, the most powerful thing you can do at eye level is to practise the ‘Wait and See’ technique.
In the video clip you can see this exact dynamic in action. Look at how I am sitting cross-legged on the mat, at eye level with the toddler. Notice how my hands are on the toy container, but my eyes are locked on the child. I am not forcing the interaction; instead, I am waiting.
Here is how you can use this strategy at home:
Set the stage: Get down on their level with a high-interest toy that requires help (like a wind-up toy, bubbles, or a tight-lidded box with toys inside).
Create anticipation: Hold the object near your face or place your hands on it, but don’t open or activate it right away.
Lean in and wait: Lean slightly forward, open your eyes wide, adopt an expectant facial expression, and completely pause. Count to five or ten in your head. Do not say anything.
Capture the gaze: Wait for the exact moment your child looks up from the toy to meet your eyes, as if to say, ‘Well? Are you going to open it?’
Reward the eye contact: The instant they make eye contact, deliver the language reward! Model a simple, functional word like ‘Open!’, ‘Go!’, or ‘Look!’ as you immediately do the action.
By pausing and waiting at eye level, you create a ‘communication temptation’. The child learns that looking at you and engaging with your face is the key that unlocks the fun.
Making it a daily habit
You don’t need to spend hours a day sitting on the floor to see a difference. Start small by dedicating just 10 to 15 minutes of undivided, face-to-face play time each day. Turn off the television, put your phone in another room, get down on their level, and let them lead the play while you focus on being their visual communication partner.
Whether you’re opening a little toy briefcase, pushing a plastic train along a track, or stacking blocks, remember: your face is the best toy in the room.
Are you wondering if your toddler’s speech and language milestones are on track? At London Speech and Feeding I love helping families navigate early communication. Feel free to explore my services page and reach out directly to schedule a consultation.
Sonja McGeachie
Highly Specialist Speech and Language Therapist
Owner of The London Speech and Feeding Practice.
Find a speech and language therapist for your child in London. Are you concerned about your child’s speech, feeding or communication skills and don’t know where to turn? Please contact me and we can discuss how I can help you or visit my services page.
As speech and language therapists, some of the most effective moments in therapy don’t come from flashcards, worksheets, or even drilling sounds (though to be fair I do drill quite a lot too! needs must…😊).
By and large they happen in natural interaction — during shared attention, laughter, storytelling, and connection.
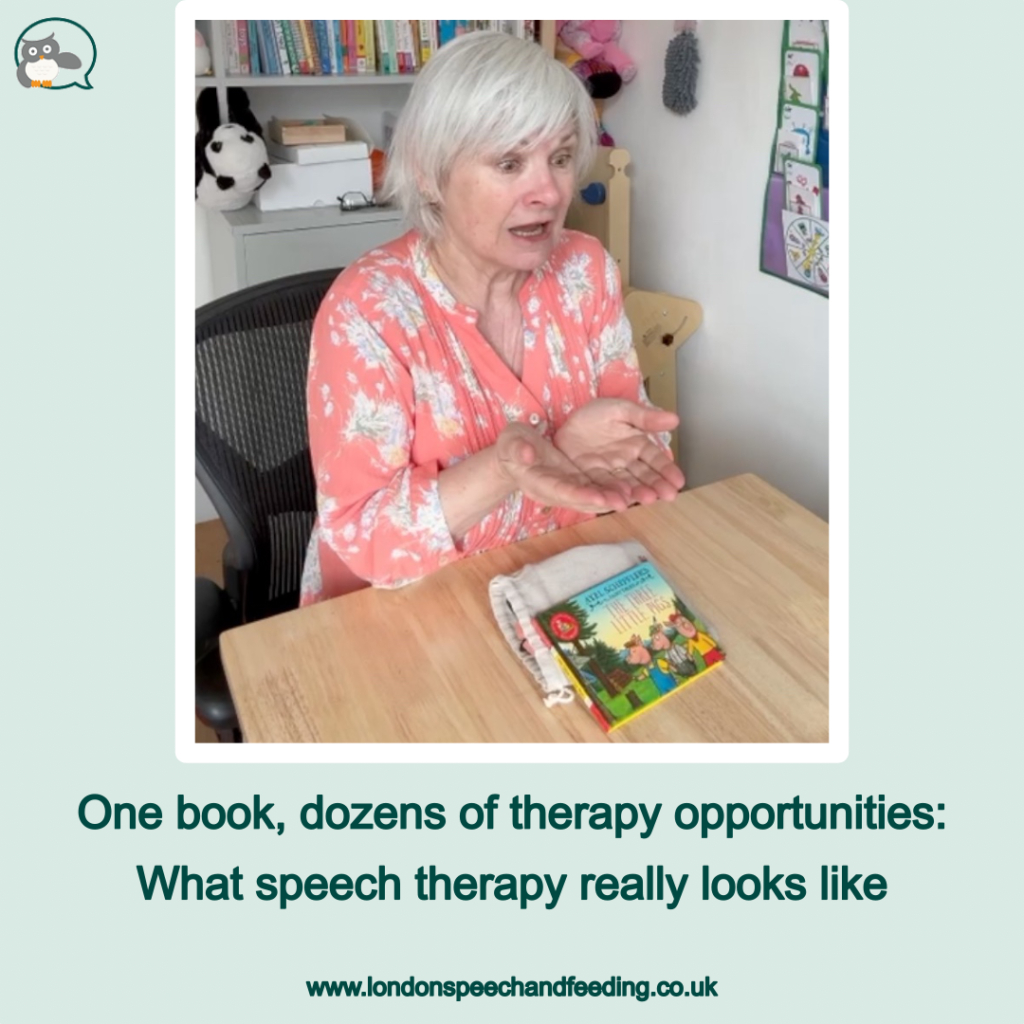
This short video clip captures that.
In under two minutes, while simply reading a book together with a three-year-old child, we naturally work on:
Speech sounds
Vowel production
Early phonological patterns
Motor planning
Signing and total communication
Visual cueing
Repetition and practice
Confidence building
And engagement through play
To many people, it may just look like ‘reading a book’.
But underneath that moment are years of specialist training, clinical decision-making, preparation, and therapeutic skill.
Therapy hidden inside play
One of the most important parts of paediatric speech therapy is knowing how to embed targets into meaningful interaction.
Books are one of my favourite therapy tools! Why: because as speech therapists we need to prepare for our child and our sessions. And having a book gives me the structure to know beforehand what kind of sounds or words might be coming up. Then I can be prepared for providing extra support for them. As you can see in this clip, I had the sound cards just there because I had anticipated what might be coming up!
A single story can provide opportunities for:
Speech sound practice
Vocabulary development
Sentence building
Turn-taking
Symbolic understanding
Attention and listening
Gesture and signing
Motor speech cueing
And social communication
In this clip, I follow my little one’s interests while carefully weaving in her individual therapy targets.
It looks relaxed and spontaneous — and it is — but it is also highly intentional.
Catching opportunities in the moment
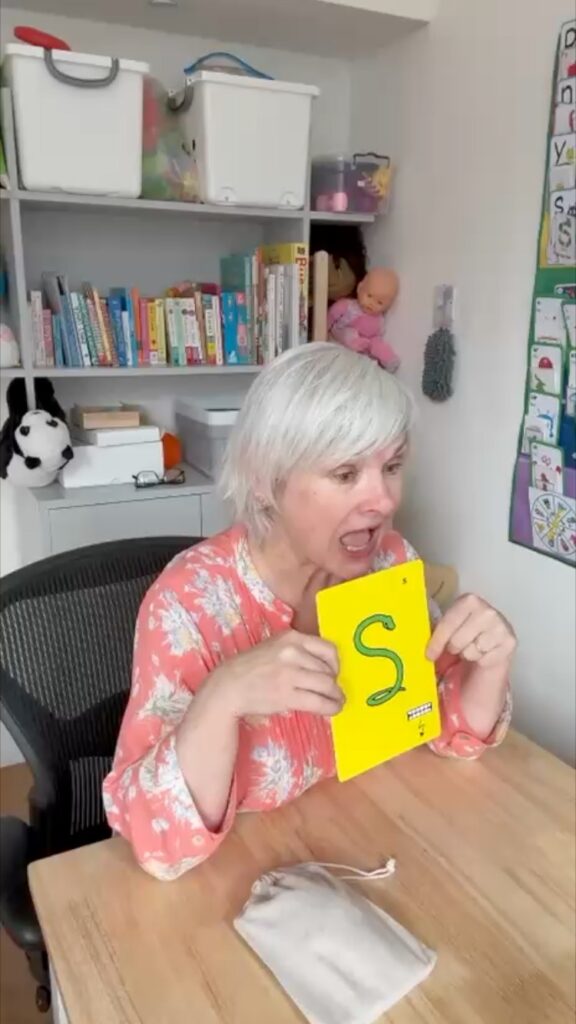
One lovely example in the clip is when she says ‘yes’.
She is now starting to say the final /S/ sound, so I immediately model and draw attention to it using the ‘snake sound’ visual cue, giving her positive feedback that she can now also try using this sound at the start of words.
My gently shaping the word ‘yeSSSS.’ gives her:
Auditory feedback
Visual support
And an achievable opportunity to try again
A few seconds later, we naturally practise it again.
That’s responsive therapy.
Speech therapists are constantly listening, analysing, adapting, and deciding:
When should I model?
When should I pause?
When should I repeat?
When should I let it go?
How can I keep confidence high while still targeting speech?
These decisions happen in seconds.
Working on speech without ‘stopping the play’
Another moment in the clip focuses on the word ‘out’, where the vowel sound is one of her speech targets.
Then we move into practising the word ‘open’, a word she has previously found difficult.
Within this one word, we can support:
Sequencing
Motor planning
Lip shape
Vowel production
And speech sound accuracy
We also briefly practise the /K/ sound — a sound produced at the back of the mouth which can be particularly tricky to produce.
Instead of explaining it verbally (which is often too abstract for young children), I use:
Visual demonstration
Exaggerated mouth movements
Gesture/sign support
And playful modelling
Children learn through seeing, hearing, doing, and experiencing.
That is why Speech Therapists use multiple layers of cueing simultaneously.
Why I use signs alongside speech
Throughout the clip, I also use signs such as ‘book’ and ‘pig’.
Using signs does not stop children talking.
In fact, for many children, signs:
Reduce frustration
Support understanding
Increase participation
Reinforce vocabulary
And help bridge the gap while speech is developing
Communication always comes first.
Speech is only one part of communication.
When children feel successful communicating, they are far more likely to keep trying.
The skill behind ‘natural’ therapy
One thing I often hear from parents is:
‘You make it look so easy.’
That is actually one of the biggest compliments a therapist can receive. (Though we also often feel we need to justify our very existence with these thoughts because we don’t just play/just read but we know it can look like that!) 😊 this is the reason for this blog…
High-quality paediatric therapy should feel warm, playful, responsive, and natural.
But underneath that natural interaction is:
Clinical knowledge
Phonological analysis
Motor speech understanding
Language development expertise
Sensory awareness
Relationship-building
And careful session planning
Before this session even began, I already knew:
Which speech patterns to target
Which words would likely appear in the book
What visual cues might help
Which signs to model
And how to adapt depending on the child’s responses
That preparation allows therapy to stay child-led without losing therapeutic focus.
Following the child while leading the therapy
The best therapy is rarely rigid.
Children do not learn communication through pressure or endless correction. They learn through interaction.
That is exactly what this short clip demonstrates.
One book. One conversation. Hundreds of tiny therapeutic decisions.
And all within a joyful moment shared together.
Because good speech therapy should never feel like hard work for a child.
It should feel like connection, confidence, success — and fun.
If you’re concerned about your child’s speech and language or wondering whether they might benefit from speech therapy, feel free to get in touch.
Sonja McGeachie
Highly Specialist Speech and Language Therapist
Owner of The London Speech and Feeding Practice.
Find a speech and language therapist for your child in London. Are you concerned about your child’s speech, feeding or communication skills and don’t know where to turn? Please contact me and we can discuss how I can help you or visit my services page.