When ‘star’ sounds like ‘dar’: Understanding speech sound disorders and the path to clearer speech
If your child says ‘dar’ instead of ‘star’, you might be wondering if they will simply outgrow it or if they require specialised support. While ‘cluster reduction’—dropping one of the sounds in a blend—is a normal part of learning to talk, we typically expect these sounds to lock into place by age four years. If these errors persist as a child approaches school age, it often signals a speech sound delay that may now no longer pass without help. As a Speech and Language Therapist, I specialise in helping children bridge this gap using evidence-based techniques like backward chaining.
This isn’t about constant correction; it’s about providing the right clinical scaffolding to move a child from ‘frustrated’ to ‘fluent’ before they hit those critical early school years.
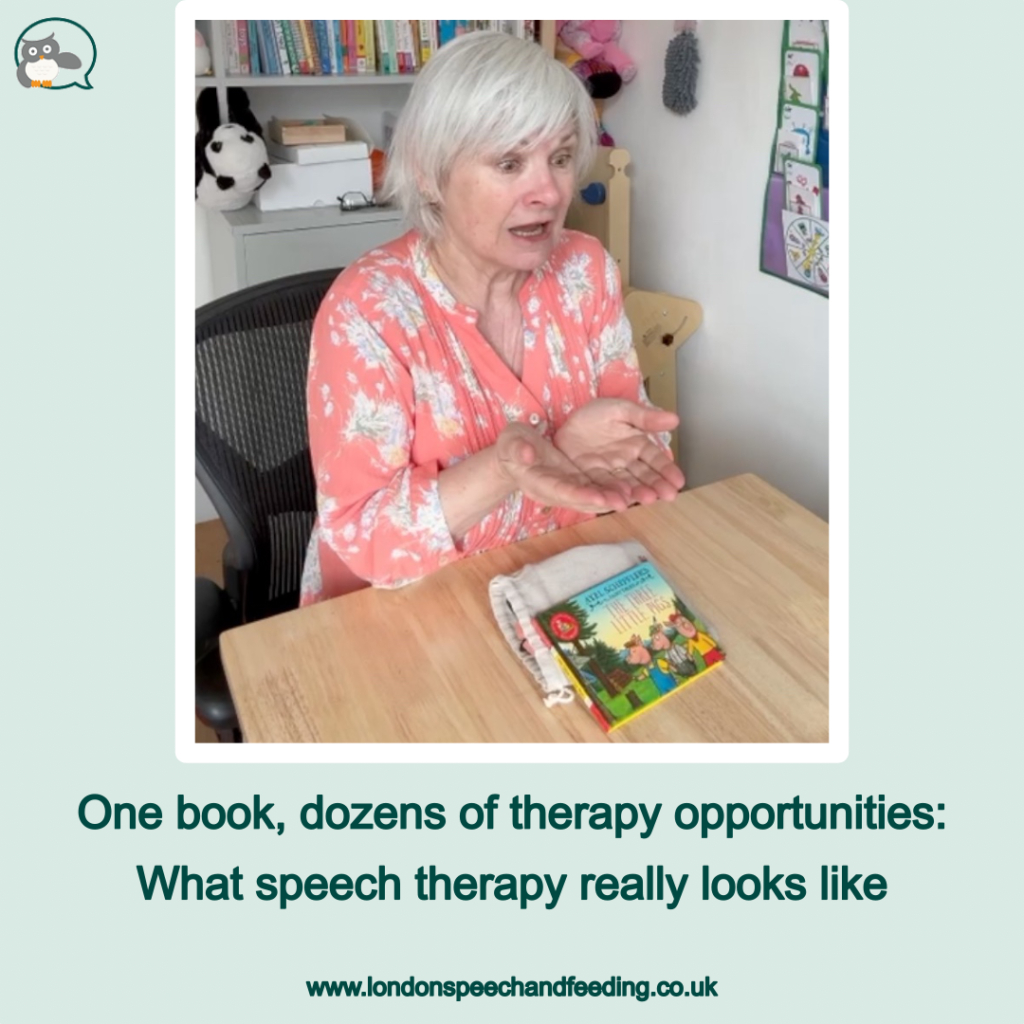
Dropping sounds from words is a common feature of speech sound difficulties, and while it can look small on the surface, it can have a big impact on how clearly a child is understood. In this short video clip, I’m working with a child on an /ST/ sound cluster, demonstrating how I use an evidence-based speech therapy technique called backward chaining to help children build clearer speech with confidence.
What’s actually happening when a child drops the ‘S’?
Clusters like /ST/, /SP/, and /SK/ are tricky. They require:
- precise timing
- careful airflow
- and the ability to blend sounds smoothly
For many children, especially those with speech sound difficulties, this is a big ask.
So instead of hearing:
‘star’
we might hear:
‘tar’ or ‘dar’
This isn’t laziness or refusal. It’s the child simplifying the word to make it manageable.
Why I don’t start by saying ‘say star’
Telling a child to ‘just add the S’ rarely works.
Instead, I meet them where they are already successful.
In this clip, the child can already say ‘dar’ clearly. That’s our starting point.
Backward chaining: building speech from success
Backward chaining means we:
- Start with the part of the word the child can already say
- Gradually add the missing sound
- Keep the child feeling successful at every step
So rather than jumping straight to ‘star’, we:
- secure the ending
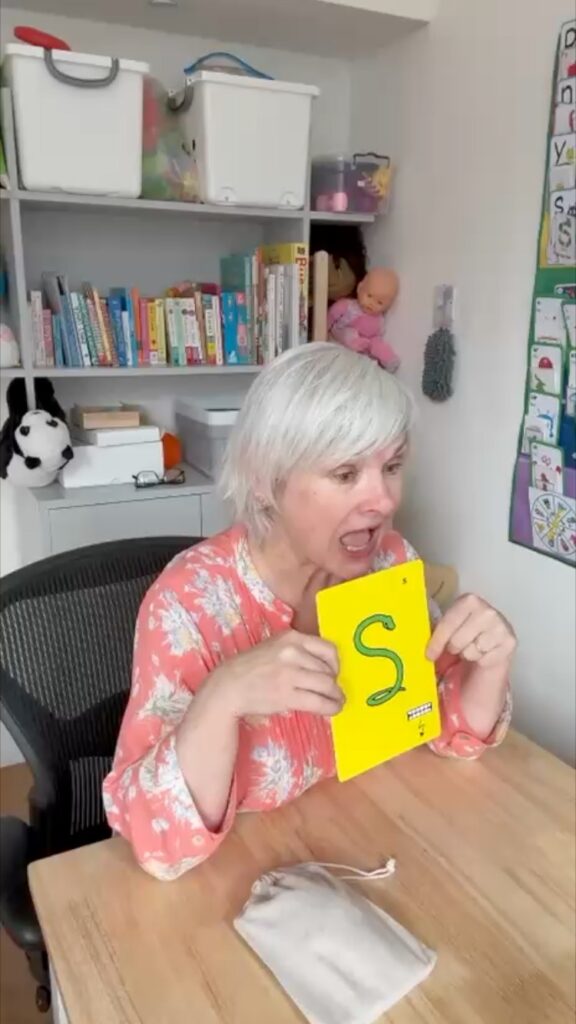
- gently introduce the /S/
- and blend it in a way that feels achievable
This approach reduces frustration, builds confidence, and helps the sound stick not just in the therapy room, but out in the real world.
Why this matters beyond one word
This isn’t just about saying ‘star’.
It’s about:
- teaching the mouth a new movement pattern
- giving the brain time to organise the sound sequence
- and helping the child feel capable, not corrected
When therapy feels safe and successful, children are far more likely to generalise their new sounds into everyday speech.
Speech therapy works best when children feel supported not tested.
If your child struggles with speech clarity
If your child:
- drops sounds from words
- avoids longer or trickier words
- or becomes frustrated when they’re not understood
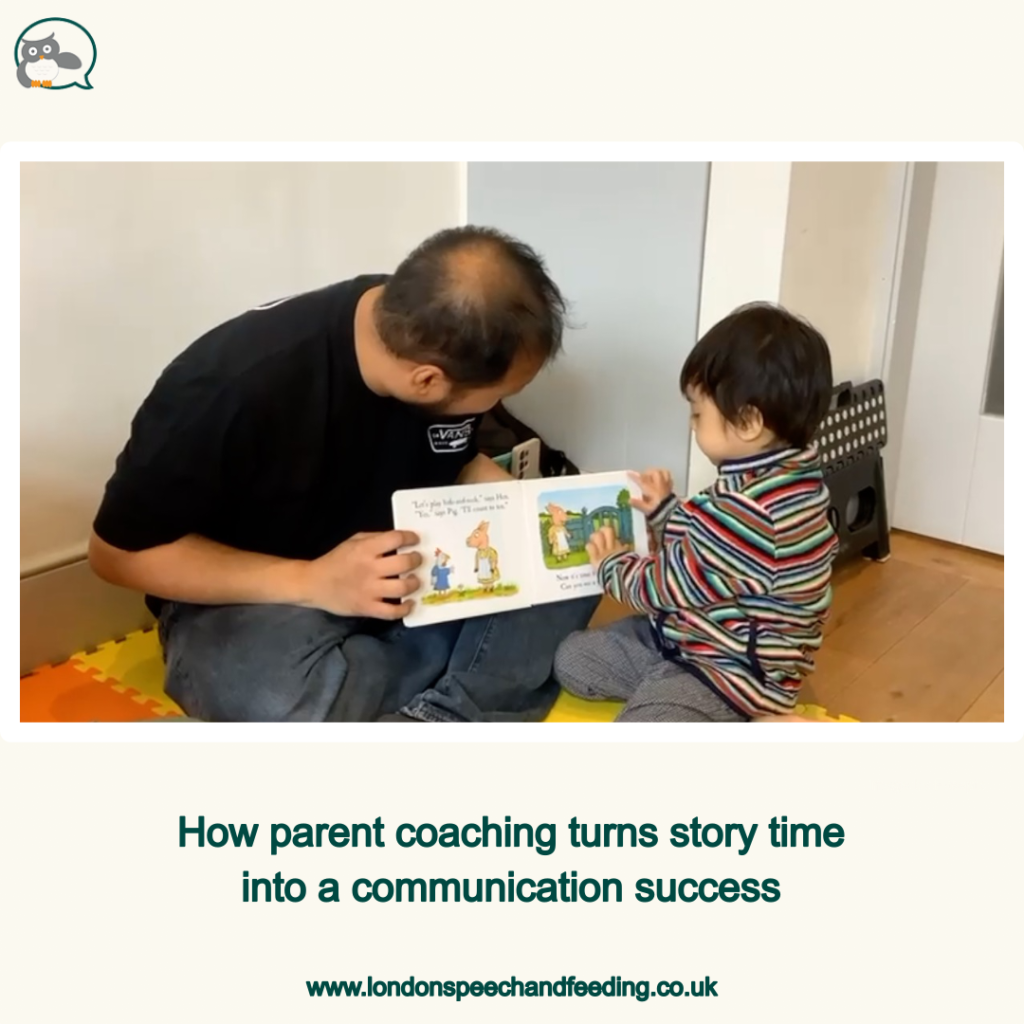
This is the kind of work I do every day building speech step by step, in a way that respects each child’s pace and strengths.
Support can be gentle, effective, and empowering.
If you’d like to learn more about how speech therapy can support your child, you’re always welcome to get in touch.

Sonja McGeachie
Highly Specialist Speech and Language Therapist
Owner of The London Speech and Feeding Practice.



Find a speech and language therapist for your child in London. Are you concerned about your child’s speech, feeding or communication skills and don’t know where to turn? Please contact me and we can discuss how I can help you or visit my services page.