Could mouth breathing be affecting your child’s speech, sleep and development?
Understanding Orofacial Myofunctional Disorders (OMDs)
Many parents contact me at London Speech and Feeding because they are worried about their child’s speech. Perhaps their child is difficult to understand, has a persistent lisp, struggles with feeding, snores at night, or always seems to have their mouth open.
What many families don’t realise is that these concerns may all be connected.
Increasingly, research and clinical experience are highlighting the important role of Orofacial Myofunctional Health, the way the muscles of the face, mouth, tongue and airway work together to support breathing, eating, sleeping and communication.
When these muscles are not functioning optimally, children may develop what are known as Orofacial Myofunctional Disorders (OMDs).
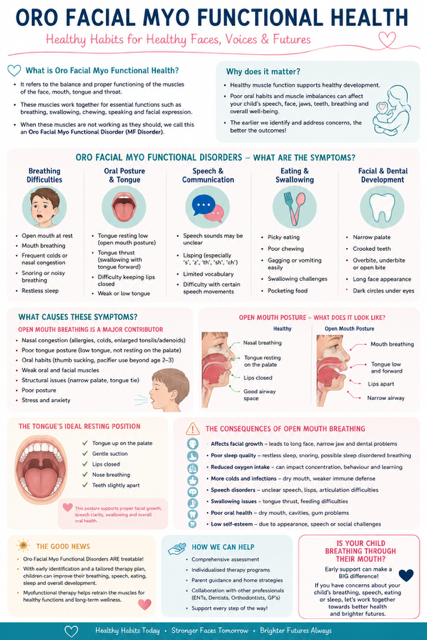
What Is Orofacial Myofunctional Health?
Orofacial Myofunctional Health refers to the healthy function and coordination of the:
- lips
- tongue
- jaw
- cheeks
- facial muscles
- airway.
These structures play a vital role in:
When everything is working well, the lips remain gently closed at rest, breathing occurs through the nose, and the tongue rests against the roof of the mouth.
This seemingly simple posture has a profound influence on how a child’s face, teeth and airway develop.
What is an Orofacial Myofunctional Disorder?
An Orofacial Myofunctional Disorder occurs when there is an abnormal pattern of muscle function involving the face, mouth, tongue or airway.
Children with OMDs may experience difficulties with:
- speech
- feeding
- swallowing
- sleep
- breathing
- dental development
- facial growth.
In many cases, these difficulties are linked to chronic mouth breathing.
Signs your child may have an Orofacial Myofunctional Disorder
Breathing and sleep signs
- mouth open at rest
- mouth breathing during the day
- snoring
- noisy breathing
- restless sleep
- frequent waking
- dark circles under the eyes
- chronic congestion
- fatigue despite a full night’s sleep.
Speech signs
- lisping
- unclear speech
- distorted speech sounds
- difficulty producing certain sounds
- persistent articulation difficulties
- reduced speech intelligibility.
Feeding and swallowing signs
- picky eating
- messy eating
- food remaining in the cheeks
- gagging easily
- difficulty chewing
- long mealtimes
- tongue thrust swallowing.
Facial and dental signs
- narrow palate
- crowded teeth
- open bite
- overbite
- underbite
- long face appearance
- receding chin
- poor lip seal.
If several of these signs sound familiar, a comprehensive assessment may be worthwhile.
Why does mouth breathing matter?
Many parents assume mouth breathing is simply a habit.
In reality, mouth breathing is often a symptom that something is preventing efficient nasal breathing.
Common causes include:
- enlarged tonsils
- enlarged adenoids
- allergies
- chronic nasal congestion
- recurrent infections
- structural airway differences
- tongue tie
- prolonged dummy use
- thumb sucking
- poor oral posture.
When nasal breathing becomes difficult, children naturally begin breathing through their mouths.
Over time, this can affect how the face, jaws and airway develop.
What does healthy oral posture look like?
Healthy oral posture is surprisingly simple:
- lips
- gently closed
- tongue
- resting against the roof of the mouth
- teeth
- slightly apart
- breathing
- through the nose.
This posture helps guide healthy jaw growth, facial development and airway formation.
Think of the tongue as a natural orthodontic support system. When it rests in the correct position, it helps shape the upper jaw and supports healthy facial growth.
The consequences of chronic mouth breathing
1. Speech difficulties
Children who breathe through their mouths often have altered tongue posture and reduced oral stability.
This can contribute to:
- lisping
- distorted sounds
- reduced speech clarity
- difficulty learning new speech sounds.
2. Feeding and swallowing difficulties
A low tongue posture may affect:
- chewing efficiency
- swallowing patterns
- food management
- oral motor coordination.
Many children develop a tongue thrust swallow, where the tongue pushes forward instead of moving efficiently during swallowing.
3. Poor sleep quality
Mouth breathing can contribute to:
- snoring
- restless sleep
- frequent waking
- daytime fatigue
- reduced concentration.
Poor sleep can have a significant impact on learning, behaviour and emotional regulation.
4. Changes to facial growth
Over time, chronic mouth breathing may influence:
- jaw development
- facial proportions
- dental alignment
- airway size.
This can result in:
- narrow palates
- crowded teeth
- long facial appearance
- increased orthodontic needs.
5. Oral health concerns
The nose acts as a natural filter and humidifier.
When children breathe through their mouths:
- The mouth becomes dry.
- Saliva protection is reduced.
- Risk of tooth decay increases.
- Gum health may be affected.
Why this matters for speech therapy
Speech does not develop in isolation.
The tongue, lips, jaw and airway work together to support clear communication.
At London Speech and Feeding, we look beyond speech sounds alone.
A child who presents with:
- persistent speech difficulties
- lisping
- feeding challenges
- open mouth posture
- snoring
- poor sleep
may benefit from an assessment that explores underlying orofacial myofunctional factors.
Addressing these foundations can often support more effective progress in speech and feeding therapy.
How London Speech and Feeding can help
A comprehensive assessment may include observation of:
- breathing patterns
- lip posture
- tongue posture
- swallowing function
- feeding skills
- speech sound development
- sleep concerns
- oral structures.
Where appropriate, recommendations may include:
- orofacial myofunctional therapy
- speech therapy
- feeding therapy
- home programmes
- ENT referral
- orthodontic referral
- collaborative multidisciplinary support.
The good news
Orofacial Myofunctional Disorders are often highly treatable when identified early.
Supporting healthy breathing, tongue posture and oral muscle function can positively influence:
If your child regularly breathes through their mouth, snores, struggles with speech clarity or has feeding difficulties, a specialist assessment may help identify the underlying cause.
At London Speech and Feeding, we are passionate about looking beyond symptoms and understanding the whole child. Contact me!
Sometimes the key to clearer speech starts with a simple question:
‘Is my child breathing through their nose?’

Sonja McGeachie
Highly Specialist Speech and Language Therapist
Owner of The London Speech and Feeding Practice.
Frequently Asked Questions
Can mouth breathing cause speech problems?
Yes. Mouth breathing can alter tongue posture, lip strength and oral stability, which may contribute to articulation difficulties and lisps.
Should I be worried if my child snores?
Regular snoring is not considered normal in children and may indicate airway obstruction or sleep-disordered breathing.
Can enlarged tonsils affect speech?
Yes. Enlarged tonsils may affect resonance, tongue positioning, swallowing and breathing patterns.
What age can children be assessed?
Children of all ages can be assessed if parents have concerns about speech, feeding, breathing or oral development.
What is Orofacial Myofunctional Therapy?
Orofacial Myofunctional Therapy focuses on improving breathing patterns, tongue posture, lip seal and oral muscle function to support overall health and development.



Find a speech and language therapist for your child in London. Are you concerned about your child’s speech, feeding or communication skills and don’t know where to turn? Please contact me and we can discuss how I can help you or visit my services page.