Following your child’s lead: A playful path to AAC success
Unlocking playtime: A guide to child-led learning
Does your child struggle to focus on toys or activities? Do they dart away as soon as you approach? You’re not alone!
The key to unlocking your child’s potential lies in following their lead. Let them guide the play session, and watch their engagement and focus soar.
Why Child-Led Play Works:
- Empowerment: Children feel in control, sparking their curiosity and motivation.
- Focused attention: They’ll stay engaged with activities for longer periods.
- Reduced frustration: By stepping back and observing, you eliminate the pressure and stress that often comes with directed play.
How to Implement Child-Led Play:
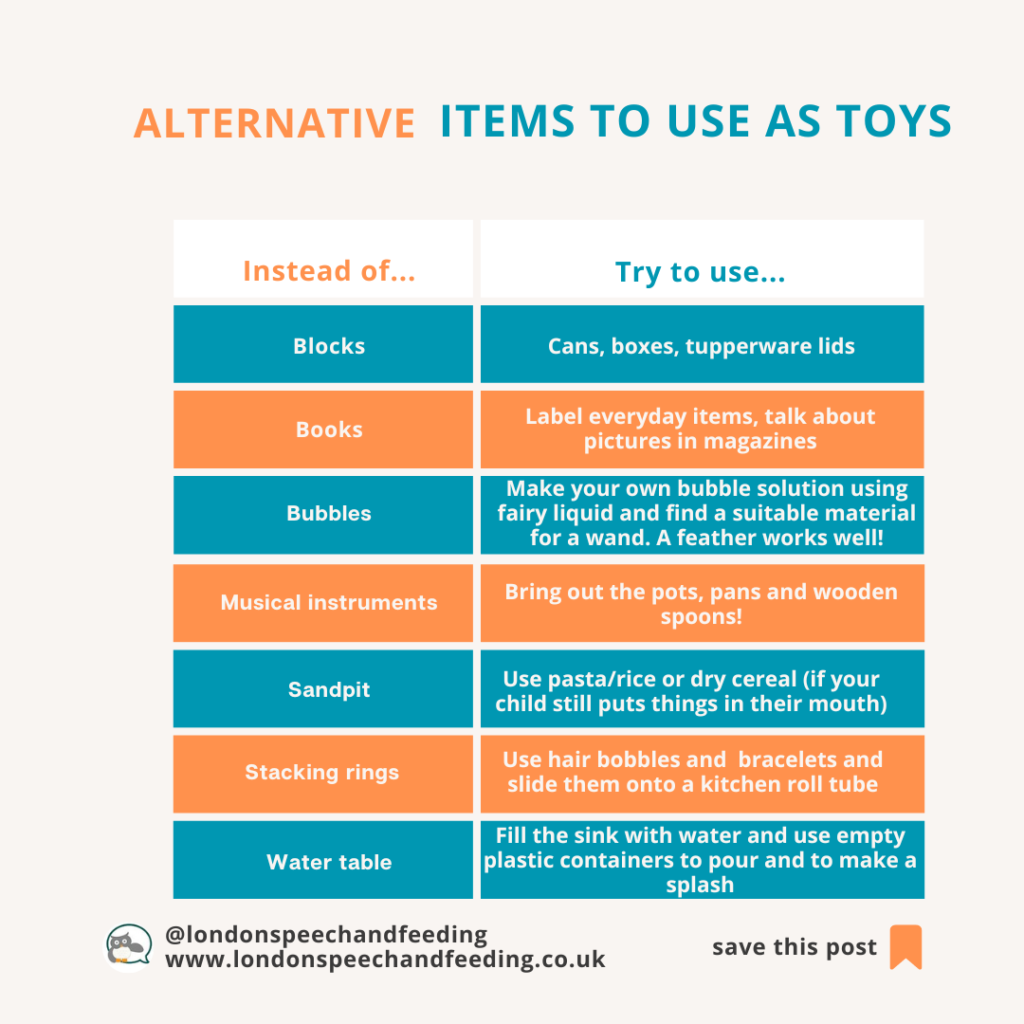
- Prepare the environment: Set out a limited selection of engaging toys.
- Observe and wait: Sit back, watch, and listen to your child’s interests.
- Embrace the moment: Resist the urge to direct or question; simply enjoy the process.
Remember: This simple approach can transform playtime and support your child’s development. Give it a try for a week and see the difference!
#OWLing #hanenmorethanwords
Observe, Wait, Listen. It’s a powerful formula for unlocking your child’s potential.
You will likely see:
- Your child will stay put with any toy for longer whilst you are near them.
- Your child will tolerate you being nearby and he/she won’t move away.
- Your child will start giving you brief glances of enjoyment, or perhaps they will hand things to you, or they might take your hand and lead it to something that needs opening etc.
- In other words, you will see that there suddenly is JOINT PLAY. Yes, granted it may not be according to your adult agenda, but there will be more togetherness than there was before. And this is the START of communication and social engagement.
USE Core words and a coreboard — to help your child understand the power of words
Core words are the building blocks of communication. Try using a coreboard like the one below, they are versatile and can be used in countless ways. By modelling these words naturally during play, you expose your child to their meaning and function in context. This approach is far more effective than isolated drill and practice, more powerful than flashcards!

A Winning Combination
Combining child-led play and AAC modelling creates a magic effect. To summarise:
- Increased engagement: When you follow your child’s lead, they are more likely to be engaged and receptive to learning. This creates optimal conditions for introducing AAC core words.
- Natural learning: By modelling AAC core words in the context of play, you help your child understand their meaning and purpose naturally. This fosters generalisation and spontaneous use.
- Building relationships: Shared play experiences strengthen the bond between you and your child. This trust and connection are essential for successful communication.
- Reduced pressure: Modelling AAC core words without expectation removes the pressure to produce language. This allows your child to explore communication at their own pace.
- Expanded vocabulary: As your child becomes more comfortable with AAC, they will begin to incorporate core words into their own communication. This leads to vocabulary growth and increased independence.
Practical Tips
- Observe and respond: Pay close attention to your child’s interests and actions. Respond to their cues with enthusiasm and support.
- Keep it simple: Start with a few core words and gradually introduce new ones as your child’s skills develop.
- Be patient: Language learning takes time. Celebrate small successes and avoid frustration.
- Have fun: Remember, play is supposed to be enjoyable for both you and your child. Relax and have fun together!
Example:

Let’s say your child is playing with a pop-up toy like you see me do in the above photograph. Here, I followed my child’s lead by waiting to see what she wanted to do with the toy. You are now OWLING! (Observe Wait and Listen)
Once I noticed that there was repetitive opening of the flaps going on I then pointed to OPEN and MORE on the board, as I said: ‘let’s OPEN this one’ / let’s see MORE animals’ / ‘MORE cow! it says moo!’ ‘OPEN another one’ and so on.
Important to know, we are not expecting our child to respond verbally or with AAC, but we are providing language input and demonstrating how these words can be used with enthusiasm.
Naturally in time your child will look at the board and at your pointing and they will eventually want to copy you!
By incorporating these strategies into your daily interactions, you can create a supportive environment that fosters language development and communication growth. If you would like more guidance please get in touch and book in for a consultation, some individual therapy and/ or some parent coaching.
I look forward to supporting you. Please contact me and let’s see how.

Sonja McGeachie
Early Intervention Speech and Language Therapist
Feeding and Dysphagia (Swallowing) Specialist The London Speech and Feeding Practice
The London Speech and Feeding Practice
Find a speech and language therapist for your child in London. Are you concerned about your child’s speech, feeding or communication skills and don’t know where to turn? Please contact me and we can discuss how I can help you or visit my services page.