
Using AAC – Augmentative and Alternative Communication for non-verbal and early verbal children

Your Speech Therapist might have been advising you to introduce words to your child with the help of a CORE BOARD. What on earth is she talking about and why would we want to do this, I hear you think – and in fact this is what I get asked a lot, as I often do recommend using Core Boards.
Core boards belong to the category of Augmentative and Alternative Communication (AAC ) and they can be really useful for:
- Children or adults who cannot speak at all or who are very hard to understand.
- Children who are slow to speak and have difficulty expressing themselves verbally, due to genetic conditions as Down Syndrome, Verbal dyspraxia, Autism or any other learning difficulty that means a child is slow to develop speech.
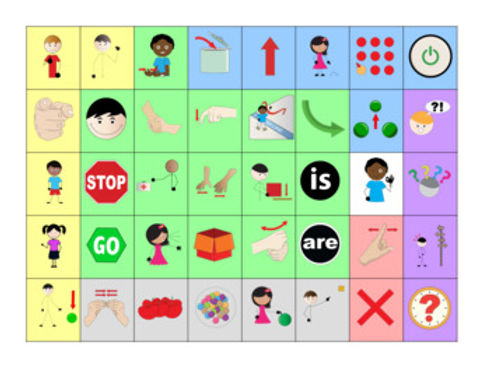
Here is what a Core board might look like, in fact this is one that I love to use. It is made by Beautiful Speech Life, there are a ton of similar boards out there for free. I have also made my own, you can check it out on my Instagram feed.
What is Core Vocabulary/ Core words?
Core vocabulary consists of the most common words used by children throughout a day. In 2003 Banajee and Dicarlo et al found that 50 % of pre-schoolers in their project used nine words consistently across their daily play and meal routines. These words are Core words and are typically the ones you can see on a board, like the one above.
How To Use It
Adults always first need to consistently model and show their child how to use a board. This is key! For example: Adult can point to “YOU” “WANT” ‘MORE” and then point to the cup of Water on the counter. Child could then reply either by shaking his/her head and/or pointing to “NOT” which also stands for “NO”. Then adult can point to “NOT” “MORE” and do an OK sign as well. Eventually Child can initiate a request and point to “I” “ WANT” “MORE” and then point to the cup on the counter.
This is not as cumbersome or limited as it first sounds or appears. Here’s why: As adult you can talk normally and, of course, many words you are using will not be on this board. But some will be, and you will be surprised how many you can find when you start using it. So you could say quite normally: Hey lovely (name of your child) would YOU LIKE some MORE water? The words in capital are on the board which you can point to as you speak normally. Basically, you are showing/saying to your child: “We can speak and these are the pictures we can use to help us; We call this TOTAL COMMUNICATION, as communication is so much more than just words! Great communication can be silent, where we use our facial expression, our smile, our eyes, our hand gestures, body movements and yes, of course, words. But when words fail us, these boards are so helpful.
This still does not answer your original question of: why would I want to do this, I want my child to talk!? You are a SPEECH Therapist, please help my child TALK, not point to pictures, that is not what I had in mind.
Let Me Explain
When speech is difficult for a child it doesn’t mean that there is nothing to talk about! Of course, we want all our children and all people to speak because it is the easiest and most effective way of communicating, no doubt! However, sometimes this is very hard for some children and whilst we are always working towards speech where possible, we also want to make sure that whilst figuring out how to speak, your child has a MEANS TO COMMUNICATE. Using a board like this might well be a temporary strategy but whilst you are using it and working on their speech you will find a reduction in tantrums and frustration as you child is able to express themselves more effectively.
Often we find that as soon as we offer a CORE VOCABULARY like the above sample a child who has had no or very few words suddenly blossoms and starts to point to new words on the board and starts to PRACTICE USING THESE WORDS!! Practice makes perfect, right? Yes it totally does! There is lots of evidence that tells us that using Core Vocabulary Boards ENHANCE AND SUPPORT SPEECH PRODUCTION AND NOT HINDER IT. Using a board like this will only ever be helpful to your child and will never make your child “lazy” – too lazy to speak? NO SUCH THING!
Here is what one of my parents says about the core board we use with her little boy:
“the board has been a game changer, my son is a visual learner so it really helps to have the board as he associates communication so much easier this way. We have incorporated his twin sister who models it’s use and have definitely seen improvement in speech through its support and his frustration around being unable to verbally communicate at times has definitely lessened”
K Connolly, Mother of Tom (aged 3.5 years).
Reading and hearing this makes me so happy!
In addition to general core board above I also sometimes use a Core Board that is specific to an activity, such as for example BLOWING BUBBLES. Below is an example of such a board, which you can use very nicely during a bubble blowing activity and sometimes it is a nice place to start for newcomers, this can be an easy introduction. You can download this and many similar boards on www.widgit.com for free!

There is so much more to say about AAC and using Coreboards, visit my Instagram you can find a bit more information on how I use them.
Find a speech and language therapist for your child in London. Are you concerned about your child’s speech, feeding or communication skills and don’t know where to turn? Please contact me and we can discuss how I can help you or visit my services page.














