Speech Sound Challenges: A focus on /L/ and /Y/
Have you ever thought about how difficult it can be to produce certain speech sounds? Some sounds are definitely trickier than others. This is especially true for children with speech sound disorders like Childhood Apraxia of Speech (CAS).
My student with CAS has been working hard on producing the /L/ sound especially when it was followed by an /O/ or /OO/ like, ‘log’ or ‘look’. We’ve practised lots and now that he’s got a good handle on /L/, he’s started replacing another difficult sound, /Y/, with it. So, ‘yes’ becomes ‘less’ and ‘yuck’ becomes ‘luck.’
This is a common pattern in speech development. Once a child masters a new sound, they may start using it in place of other sounds they find even more challenging.
Minimal Pair therapy
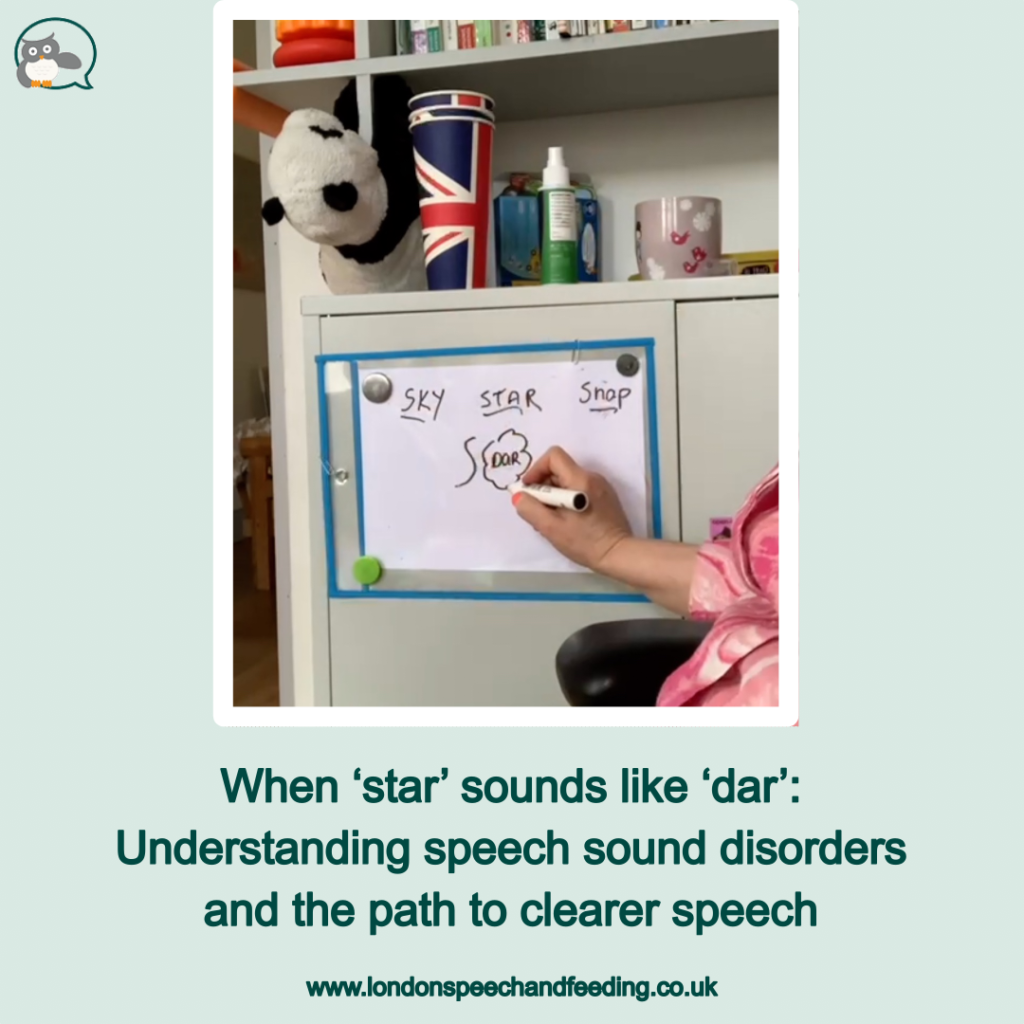
I use different evidence-based methods to help my students. And I often like to start out with phonemic awareness and then I move to contrasting the error sound with another sound to make completely different words. This approach is called ‘minimal pair’ therapy: both words are the same except for the initial/final sound which has the error sound, and this is contrasted with the correct sound.
Below is an example of this:

After we have worked on sound awareness, listening and becoming aware of small units of sound matter, then we can move to working on tongue placement and movement.
Tongue placement and movement to produce correct /L/ and /Y/ sounds
To produce these sounds correctly, the tongue needs to be in specific positions and make specific movements.
- /L/ sound:
- Tip of the tongue touches the alveolar ridge (the bony ridge behind your upper teeth)
- Sides of the tongue are raised to the sides of the upper teeth
- Airflow escapes through the sides of the tongue
- /Y/ sound:
- Tip of the tongue touches the roof of the mouth behind the alveolar ridge
- Sides of the tongue are raised to the sides of the upper teeth
- Airflow escapes through the centre of the mouth
I also use:
- Auditory bombardment: Auditory bombardment is a technique that involves repeatedly listening to a target sound. This can help children to develop a better understanding of the sound and how to produce it.
- Visual cues: Visual cues can be helpful for children who are having difficulty producing a particular sound. Here I use the image of a ‘standing tongue’ versus a ‘sitting tongue’.
- Physical cues: I use my hands to show a ‘standing tongue’ for the /L/ versus a ‘sitting tongue’ for the /Y/. But what worked even better and sadly I don’t have the video clip for it:
- Semantic cues: For example a picture of an ‘EAR’ to make the sound /Y/ so we shape the sound /EA/ to /Y/.
- Parent involvement: Parents play an important role in their child’s speech sound development by providing opportunities for them to practise their speech sounds at home. This can be done through activities such as reading books, singing songs, and playing games.
- Reinforcement: It is important to praise children for their efforts, even if they are not perfect. This will help them to feel motivated to keep practising. Important here for speech correction is concrete reinforcement: I feed back to my student what exactly they were doing correctly with their tongue or lips. Rather than saying ‘well done’, I mention what my student has just done with the tongue to change the sound: ‘I saw you lowered your tongue! That made a good /Y/’.
Another great way of reinforcing positively is to ask the student how they feel they have done? For the older ones I often ask them to self-rate their sound production out of 10. Then we can work towards the next incremental number upwards. This is very effective and gives the student control over their own work.
Please contact me if your child has speech sound difficulties.

Sonja McGeachie
Early Intervention Speech and Language Therapist
Feeding and Dysphagia (Swallowing) Specialist The London Speech and Feeding Practice
The London Speech and Feeding Practice
Find a speech and language therapist for your child in London. Are you concerned about your child’s speech, feeding or communication skills and don’t know where to turn? Please contact me and we can discuss how I can help you or visit my services page.