The /R/ sound is notoriously challenging for many children (and even some adults!). It’s one of the most complex sounds in the English language, with various pronunciations depending on its position in a word. If your child is struggling with their /R/s, you’re not alone. As Speech and Language Therapists (SLTs), we frequently work on this sound, and a key component of our therapy is focusing on proper tongue placement.
Why is the /R/ so difficult?
The /R/ sound requires precise coordination of the tongue, jaw, and lips. Unlike sounds like /P/ or /B/ that involve simple lip movements, the /R/ involves intricate tongue movements and tension. There are also different ways to produce the /R/ sound, which adds to the complexity:
Retroflex /R/: The tongue tip curls up and back towards the roof of the mouth.
Bunched /R/: The body of the tongue bunches up towards the roof of the mouth, while the tongue tip remains down.
The importance of tongue placement
Regardless of which /R/ variation is being targeted, accurate tongue placement is crucial. Even a slight deviation can result in a distorted or inaccurate sound. That’s why SLTs dedicate significant time to teaching and practising tongue positioning.
Speech therapy techniques: Focusing on the tongue
Here’s a glimpse into how I address /R/ sound difficulties, with a focus on tongue placement:
Visual aids:
Mirrors: I use a mirror to help children see their tongue movements and make adjustments.
Tongue diagrams and models: These visual tools provide a clear representation of where the tongue should be positioned.
Tactile cues:
Tongue depressors: These can be used to gently guide the tongue into the correct position.
Food-grade tools: Sometimes, I use flavoured tongue depressors or other tools to provide tactile feedback and increase awareness of tongue placement.
Auditory discrimination:
I help children distinguish between correct and incorrect /R/ sounds.
I use auditory cues and verbal feedback to reinforce proper pronunciation.
Exercises and drills:
Tongue strengthening exercises: Strengthening the tongue muscles can improve control and coordination.
Tongue placement drills: We practise positioning the tongue in the desired location and holding it there.
Sound approximation techniques: Sometimes we use other sounds to help approximate the /R/ sound. For example, I use the /L/ sound, to help achieve the correct tongue placement. Once my child has found the /L/ sound it is then a matter of pulling back just slightly to get a good /R/.
Contextual practice:
Once the child can produce the /R/ sound in isolation, we gradually introduce it into syllables, words, phrases, and sentences.
We also practise the /R/ sound in different contexts, such as at the beginning, middle, and end of words.
Tips for Parents:
Be patient and supportive: Learning the /R/ sound takes time and practice.
Practise regularly: Short, frequent practice sessions are more effective than long, infrequent ones.
Make it fun! Use games, stories, and other engaging activities to keep your child motivated.
Work with an SLT: A qualified SLT can provide personalised guidance and support.
In conclusion:
The /R/ sound can be challenging, but with targeted speech therapy and a focus on tongue placement, most children can achieve clear and accurate pronunciation.
Feeding and Dysphagia (Swallowing) Specialist The London Speech and Feeding Practice
The London Speech and Feeding Practice
Find a speech and language therapist for your child in London. Are you concerned about your child’s speech, feeding or communication skills and don’t know where to turn? Please contact me and we can discuss how I can help you or visit my services page.
Your Speech Therapist might have been advising you to introduce words to your child with the help of a CORE BOARD. What on earth is she talking about and why would we want to do this, I hear you think – and in fact this is what I get asked a lot, as I often do recommend using Core Boards.
Core boards belong to the category of Augmentative and Alternative Communication (AAC ) and they can be really useful for:
Children or adults who cannot speak at all or who are very hard to understand.
Children who are slow to speak and have difficulty expressing themselves verbally, due to genetic conditions as Down Syndrome, Verbal dyspraxia, Autism or any other learning difficulty that means a child is slow to develop speech.
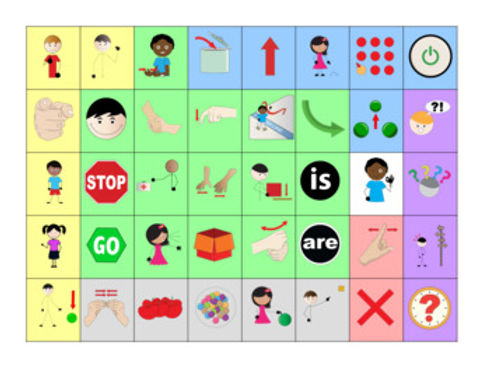
Here is what a Core board might look like, in fact this is one that I love to use. It is made by Beautiful Speech Life, there are a ton of similar boards out there for free. I have also made my own, you can check it out on my Instagram feed.
What is Core Vocabulary/ Core words?
Core vocabulary consists of the most common words used by children throughout a day. In 2003 Banajee and Dicarlo et al found that 50 % of pre-schoolers in their project used nine words consistently across their daily play and meal routines. These words are Core words and are typically the ones you can see on a board, like the one above.
How To Use It
Adults always first need to consistently model and show their child how to use a board. This is key! For example: Adult can point to “YOU” “WANT” ‘MORE” and then point to the cup of Water on the counter. Child could then reply either by shaking his/her head and/or pointing to “NOT” which also stands for “NO”. Then adult can point to “NOT” “MORE” and do an OK sign as well. Eventually Child can initiate a request and point to “I” “ WANT” “MORE” and then point to the cup on the counter.
This is not as cumbersome or limited as it first sounds or appears. Here’s why: As adult you can talk normally and, of course, many words you are using will not be on this board. But some will be, and you will be surprised how many you can find when you start using it. So you could say quite normally: Hey lovely (name of your child) would YOU LIKE some MORE water? The words in capital are on the board which you can point to as you speak normally. Basically, you are showing/saying to your child: “We can speak and these are the pictures we can use to help us; We call this TOTAL COMMUNICATION, as communication is so much more than just words! Great communication can be silent, where we use our facial expression, our smile, our eyes, our hand gestures, body movements and yes, of course, words. But when words fail us, these boards are so helpful.
This still does not answer your original question of: why would I want to do this, I want my child to talk!? You are a SPEECH Therapist, please help my child TALK, not point to pictures, that is not what I had in mind.
Let Me Explain
When speech is difficult for a child it doesn’t mean that there is nothing to talk about! Of course, we want all our children and all people to speak because it is the easiest and most effective way of communicating, no doubt! However, sometimes this is very hard for some children and whilst we are always working towards speech where possible, we also want to make sure that whilst figuring out how to speak, your child has a MEANS TO COMMUNICATE. Using a board like this might well be a temporary strategy but whilst you are using it and working on their speech you will find a reduction in tantrums and frustration as you child is able to express themselves more effectively.
Often we find that as soon as we offer a CORE VOCABULARY like the above sample a child who has had no or very few words suddenly blossoms and starts to point to new words on the board and starts to PRACTICE USING THESE WORDS!! Practice makes perfect, right? Yes it totally does! There is lots of evidence that tells us that using Core Vocabulary Boards ENHANCE AND SUPPORT SPEECH PRODUCTION AND NOT HINDER IT. Using a board like this will only ever be helpful to your child and will never make your child “lazy” – too lazy to speak? NO SUCH THING!
Here is what one of my parents says about the core board we use with her little boy:
“the board has been a game changer, my son is a visual learner so it really helps to have the board as he associates communication so much easier this way. We have incorporated his twin sister who models it’s use and have definitely seen improvement in speech through its support and his frustration around being unable to verbally communicate at times has definitely lessened”
K Connolly, Mother of Tom (aged 3.5 years).
Reading and hearing this makes me so happy!
In addition to general core board above I also sometimes use a Core Board that is specific to an activity, such as for example BLOWING BUBBLES. Below is an example of such a board, which you can use very nicely during a bubble blowing activity and sometimes it is a nice place to start for newcomers, this can be an easy introduction. You can download this and many similar boards on www.widgit.com for free!
There is so much more to say about AAC and using Coreboards, visit my Instagram you can find a bit more information on how I use them.
Find a speech and language therapist for your child in London. Are you concerned about your child’s speech, feeding or communication skills and don’t know where to turn? Please contact me and we can discuss how I can help you or visit my services page.
If you’ve found yourself wondering ‘Why can my child say a word one day, but not at all the next?’ it might be that your child has a motor speech difficulty. This means the challenge isn’t that your child doesn’t know what they want to say; it’s that their brain finds it harder to plan and coordinate the movements needed for clear speech. This speech difficulty is called Childhood Apraxia of Speech (CAS)
In this post, I’ll explain what CAS can look like in 2–5 year olds, what an assessment usually involves, and what you can start doing at home to support your child without turning life into ‘speech homework all day long’.
What is childhood apraxia of speech (CAS)?
Children with CAS often have lots to communicate about (and strong ideas!) but their speech may come out as:
Unclear
inconsistent
hard to ‘copy’ on demand
frustrating for them and for you
CAS is not caused by laziness and it is not a parenting issue. It is also not something children simply ‘grow out of’ without support. But with the right therapy approach, children can absolutely build clearer speech over time.
Many families come to me after months (or years) of being told:
‘She’ll talk when she is ready’
‘He’s just shy’
‘It’s probably a speech delay’
‘It’s normal for toddlers’
And sometimes it is a general delay. But sometimes it’s something more specific, like CAS.
There’s also been a huge rise in parents seeking information online, and CAS is often mentioned alongside speech sound difficulties such as:
phonological delay (pattern-based speech errors)
articulation difficulties (one sound that won’t come out clearly)
inconsistent speech disorder
These can look similar at first glance, which is why a specialist assessment matters.
Signs of childhood apraxia of speech in 2–5 year olds
Children develop speech at different rates, and not every unclear speaker has CAS. But here are some common features that may raise a flag, especially when you notice several together.
1) Inconsistent speech errors
Your child might say the same word in different ways:
‘banana’ → nana / baba / mana
‘daddy’ → gaga / daddy / dadi
This inconsistency is one of the biggest clues.
2) Difficulty copying words on request
Some children speak more easily in natural play, but when asked ‘Say ___’, they freeze or the word becomes much harder.
3) Limited sound repertoire
They may use only a small set of consonants (like /M/, /N/, /B/, /D/) and avoid others.
4) Vowel distortions
Many children with typical delays mainly struggle with consonants. But in CAS, vowels can also sound ‘off’ or change between attempts.
5) Speech that sounds effortful
You might notice your child:
pauses between sounds
tries multiple times
looks like they’re ‘searching’ for the right mouth movement
6) Longer words are much harder
‘Car’ might be easier than ‘carry’, and ‘carry’ easier than ‘caterpillar’.
7) Prosody differences (rhythm and stress)
Some children with CAS sound a little unusual in their speech rhythm, stress, or intonation.
8) Frustration or reduced confidence
When a child is frequently misunderstood, they may:
talk less
use gestures more
become upset when asked to repeat themselves
Important note: none of these signs alone prove CAS but they are a strong reason to seek a speech assessment rather than waiting.
CAS vs phonological delay vs articulation difficulty (quick guide)
These are some of the most common questions I hear.
If it’s mainly an articulation difficulty…
A child may consistently say one sound incorrectly (for example, ‘thun’ for ‘sun’- lisp- but everything else is developing well.
If it’s mainly a phonological delay…
You might notice clear patterns, like:
leaving off the ends of words (‘ca’ for ‘cat’)
swapping back sounds for front sounds (‘tar’ for ‘car’)
Patterns are often consistent and respond well to phonology-based therapy.
If it might be CAS…
Speech often feels less predictable, harder to imitate, and more impacted by word length and complexity.
If you’re unsure, that’s completely normal, and exactly why assessment matters.
What happens in a CAS assessment?
A high-quality speech assessment for possible CAS usually includes:
1) Parent discussion and developmental history
We talk about:
pregnancy and birth history (where relevant)
feeding history
early sounds and babbling
first words and how speech has progressed
family history of speech/language needs
2) A speech sound assessment
Your child might be shown pictures or play-based prompts so we can hear:
what sounds they can say
what they simplify
whether errors are consistent or inconsistent
3) An oral-motor and movement check
This isn’t about ‘strength’. It’s about coordination and planning. We look at how your child manages speech movements and transitions.
4) Stimulability testing
This means: how easily can your child learn a new sound or word with support?
For CAS, we often explore how they respond to:
slowed-down speech
visual cues
rhythm/tapping
short, simple syllable shapes
5) Functional communication and confidence
We look at how speech impacts daily life:
being understood at nursery
joining in with peers
asking for help
managing emotions when misunderstood
At the end, you should leave with:
a clear explanation of what we think is going on
a therapy plan
practical home strategies
realistic next steps
What parents can do at home
Here are CAS-friendly strategies you can start right away.
1) Choose ‘power words’
Pick 1–2 words that matter most in your child’s daily life, such as:
more
help
mummy
again
stop
open
These words are motivating and functional.
2) Keep it short and successful
For many children with CAS, the goal is quality over quantity.
Try five minutes a day rather than 30 minutes of struggle.
3) Support speech with rhythm
Some children benefit from:
tapping a beat on the table
clapping syllables
using a gentle ‘marching’ rhythm
This can help the brain organise the sequence of movements.
4) Celebrate approximations
If your child says ‘moh’ for ‘more’, that’s communication!
We want them to feel:
safe
understood
proud to try again
Confidence is a key part of progress.
A short parent story (anonymised)
One mum said to me:
‘We kept being told to wait. But I could see my child understood everything; they just couldn’t get the words out. Once we had an assessment and a plan, it felt like we finally knew what to do. The biggest change was his confidence. He started trying more.’
When should you seek support?
You don’t need to wait until school.
It’s worth getting an assessment if your child is:
hard to understand compared with peers
becoming frustrated or withdrawing from talking
inconsistent with words they used to say
struggling to imitate speech sounds
showing signs that match CAS
Early support can reduce stress for the whole family and help your child feel successful in communication.
Here’s how I can help:
✅ A detailed speech assessment (including whether CAS is likely)
✅ A clear therapy plan with realistic goals
✅ Practical home strategies you can use immediately
✅ Support for nurseries and schools (where needed)
✅ In-person sessions in North-West London and online options
Your child is communicating the best way they can, and with the right support, speech can become easier, clearer, and more confident.
Sonja McGeachie
Highly Specialist Speech and Language Therapist
Owner of The London Speech and Feeding Practice.
Find a speech and language therapist for your child in London. Are you concerned about your child’s speech, feeding or communication skills and don’t know where to turn? Please contact me and we can discuss how I can help you or visit my services page.
Childhood Apraxia of Speech (CAS) is a complex neurological disorder that affects a child’s ability to plan and coordinate the movements necessary for speech production. Children with CAS often have difficulty with articulation, prosody, and fluency, making it challenging for them to communicate effectively. While there is no cure for CAS, speech and language therapy can significantly improve a child’s communication skills and overall quality of life. Understanding the principles of motor learning is crucial for both parents and speech therapists to support children with CAS on their speech journey.
What is MOTOR LEARNING?
Motor learning refers to the process of acquiring and refining new skills through practice and experience. This applies to all aspects of movement, including speech production. The brain constantly receives sensory information about the movements being made and adjusts them based on the desired outcome. A breakdown or interruption of this process can make it difficult for children to plan, sequence, and coordinate the intricate movements involved in speech.
What key principles do we use in speech and language therapy for motor learning?
Task Specificity: Speech Therapy activities that directly target the specific speech sounds or skills your child is working on. For example, if your child is struggling with /p/, practising isolated /p/ sounds, words with /p/, and phrases with /p/ would be most beneficial.
Massed vs. Distributed Practice: We consider the optimal amount and distribution of practice sessions throughout the day. Massed practice involves concentrated practice in a single session, while distributed practice spreads practice sessions throughout the day. The best approach depends on the individual child’s learning style and attention span.
Feedback: We provide clear and immediate feedback to help your child understand the accuracy and effectiveness of their attempts. This feedback can be auditory, visual, or touch based.
Error Correction: We aim to gently correct errors so that we can help your child refine their movements and avoid developing bad habits. The focus is on providing specific cues and guidance rather than simply pointing out mistakes.
Variety and Progression: We gradually introduce new challenges and variations in speech therapy activities to prevent plateaus and maintain motivation.
Motivation and Engagement: A big part of our work is to make therapy sessions fun and engaging to keep your child motivated and actively participating. We use games, songs, and activities that your child enjoys while incorporating targeted practice opportunities.
What about home work?
Yes we need your help and here are some examples of how this could look:
Task Specificity: During story time, focus on practising target sounds present in the story. Have your child repeat words or phrases containing the sound and encourage them to identify the sound in other words.
Massed vs. Distributed Practice: Instead of one long practice session, try shorter, more frequent sessions throughout the day. This can help maintain focus and prevent fatigue. It is recommended to go for 100 repetitions of the target sound per day, every day in between the sessions. We can decide together how you can best do that through either massed or distributed practice. We can decide after the session.
Feedback: Use a mirror to provide visual feedback on lip and tongue placement during sound production. Record the child’s speech and play it back to help them self-monitor their accuracy.
I quite like this mirror below but any table top mirror will work as long as it is not too small. Your child should see their whole face easily.
Error Correction: If the child makes an error, gently model the correct sound or movement without shaming or criticising. Provide specific cues such as ‘lips together’ for /p/ or ‘tongue up’ for /t/.
Variety and Progression: We will guide you on exactly what words to practise so this is something you need not worry about.
Motivation and Engagement: Use games, songs, and activities that your child enjoys. Play a game of ‘I Spy’ focusing on words with the target sound or create silly sentences with the sound to make practice fun.
Let’s work together!
It is crucial for parents, therapists, and other caregivers to work collaboratively to ensure a consistent and comprehensive approach to supporting your child’s speech development. Speech and Language Therapists can provide guidance and resources on implementing these principles at home, while parents can share observations and progress updates to inform therapy sessions.
Remember, every child with CAS learns at their own pace. By understanding and applying the principles of motor learning, parents and speech therapists can create a supportive and stimulating environment that empowers children with CAS to reach their full communication potential.
Do get in touch if you would like some in-person or on-line 1:1 support with this. It can be overwhelming to figure it all out alone.
Find a speech and language therapist for your child in London. Are you concerned about your child’s speech, feeding or communication skills and don’t know where to turn? Please contact me and we can discuss how I can help you or visit my services page.
You may be questioning ‘will my child grow out of having a lisp?’ There are so many myths out there that it’s sometimes difficult to find your way out of a complex maze of information.
The good news: lisps can be successfully treated by a Speech and Language Therapist and the earlier it’s resolved, the better. We know from the evidence base that some children’s lisps will resolve and, as always, it is completely age appropriate to have this speech pattern up until aged 4 ½.
As with any speech and language targets your child will need to be motivated to practise their newly acquired techniques, at home and in other settings. They will eventually be able to generalise this skill, but it takes lots of practice. So, think carefully about if your child is ready and motivated before commencing Speech and Language Therapy.
There are essentially two ways in which your child has acquired a lisp. It’s key here to mention that parents have no blame in this.
They’ve mis-learned it and now incorrect production has become a habit
Children have difficulties organising the sounds to make a clear production
You may be surprised to realise that there are different types of lisps. But all the techniques will be the same.
Interdental lisp
When your child pushes their tongue too far forward, they will make a /th/ sound instead of /s/ and /z/
Dental lisp
This is where your child’s tongue pushes against their teeth
Lateral lisp
Air comes over the top of the tongue and down the sides
Palatal lisp
Your palate is the roof of your child’s mouth. Sometimes they will touch their palate when making certain sounds (e.g., /s/ and /z/)
It’s useful for you to know what type of lisp your child has because you can then support them to make the correct production. You’ll be able to talk about where in the mouth their tongue is and where it needs to be to produce a clear sound. Your Speech and Language Therapist will be able to help you with this.
Top therapy tips for lisps
Awareness is key. Does your child know where their tongue and teeth are (i.e., are they behind their teeth)? Do they notice the air escaping? Use a mirror so that your child can see not only themselves but also you in the mirror.
Repetition! As with most therapeutic intervention, practice makes perfect. So little and often is key!
Make sessions fun, perhaps around your child’s interests or allow them to drink from a straw
Comment on how the sound is produced (e.g., /z/ is like a bee, /s/ is like a snake)
Use tactile cues. Your child’s vocal folds vibrate when they produce a sound like /z/ but not with /s/. You could use the words ‘loud’ and ‘quiet’ to describe this.
Start with a /t/ sound and gradually elongate the sound to an /s/
Having a lisp may not be problematic for some, but for other children, it can have a significant impact on their emotional wellbeing. Intervening at an early age can prevent this from happening. We always advocate for early intervention!
Find a speech and language therapist for your child in London. Are you concerned about your child’s speech, feeding or communication skills and don’t know where to turn? Please contact me and we can discuss how I can help you or visit my services page.
One of the most important things I have learned as a paediatric speech and language therapist is this:
Children do not all learn communication in the same way.
Some children learn best through listening. Some need visual support. Some need movement and gesture. Some benefit from symbols or technology. And many children need multiple supports together before communication truly starts to develop.
That is why flexible, responsive therapy matters so much.
In this short therapy clip, I model just two simple words: ‘Go’ and ‘Up’.
But underneath those tiny moments is a combination of therapeutic strategies:
speech sound prompting
visual cueing
Makaton signing
AAC (Augmentative and Alternative Communication) modelling
repetition
motor planning support
language modelling
total communication principles.
Communication is bigger than speech alone
One of the biggest misconceptions about speech therapy is the idea that communication only ‘counts’ if a child says the word verbally.
In reality, communication comes in many forms:
speech
gesture
facial expression
signing
pointing
symbols
body language
AAC.
This is particularly true for children with:
developmental language disorder (DLD)
autism
motor speech difficulties
childhood apraxia of speech (CAS)
phonological difficulties
global developmental delay
complex communication needs.
These children often need communication to be presented through multiple pathways at once.
That is where total communication approaches become so powerful.
This is important to know: this does not confuse children. In fact, for many children, it does the opposite. It creates clarity.
Research suggests that learning signs alongside spoken language does not hinder speech development and may support overall language acquisition, communication confidence, and vocabulary growth in many children.
For many children, signs actually help speech emerge because they:
reduce communication pressure
build confidence
strengthen understanding of words.
A child who can successfully communicate is far more likely to keep attempting interaction.
The power of AAC and LAMP Words for Life
In the clip, I also model language using an electronic AAC system: LAMP Words for Life.
AAC stands for Augmentative and Alternative Communication.
AAC includes any tool that supports communication beyond speech alone, including:
picture systems
symbol boards
communication books
speech-generating devices.
LAMP Words for Life is one of my favourite AAC systems because it focuses on consistent motor patterns and meaningful language development. Because communication is not about achieving perfection. It is about connection.
And when children are given multiple ways to express themselves, they often become more confident, more engaged, and more willing to interact with the world around them.
That is the true power of total communication therapy.
Find a speech and language therapist for your child in London. Are you concerned about your child’s speech, feeding or communication skills and don’t know where to turn? Please contact me and we can discuss how I can help you or visit my services page.
The practice of wrapping or swaddling children, often referred to as ‘containment,’ has been used for centuries to soothe and comfort infants. I use this therapeutic approach with autistic children at the London Speech and Feeding Practice. While it might seem counterintuitive, the act of being tightly wrapped can provide significant benefits for children who struggle with sensory processing, emotional regulation, and communication.
Understanding sensory processing and autism
Autistic persons often experience challenges with sensory processing, which is their brain’s ability to interpret and respond to sensory information. This can lead to sensory overload or under-responsivity. Containment can be a valuable tool in helping children regulate their sensory input.
To summarise, here are some of the benefits of containment:
Sensory Regulation:
Provides deep pressure input: The tight, enveloping sensation of being wrapped can provide deep pressure input, which is calming and organising for many children.
Reduces sensory overload: By creating a controlled sensory environment, containment can help to reduce overstimulation and promote a sense of safety.
Emotional Regulation:
Containment creates a sense of security: Being wrapped tightly can mimic the feeling of being in the womb, providing a sense of security and comfort.
Facilitates calming: The deep pressure input can help to calm the nervous system and reduce anxiety.
Improved Body Awareness:
Enhances proprioception: Containment can improve the child’s awareness of their body in space, which is essential for motor development and sensory integration. I often provide extra pressure on a child’s arms and legs sticking out of the yoga mat; this helps my child understand where their limbs are in space: I can feel my legs and I can feel my arms and I can feel where they are right now, i.e. they are under Sonja’s hand, I can feel them.
Facilitates Communication – and this is obviously where I come in as a Speech and Language Therapist:
Swaddling creates a safe space: When a child feels calm and secure, they are more likely to engage in communication.
Enhances joint attention: The shared experience of being wrapped can foster joint attention, which is essential for language development. You can see this one in my highlights where I swaddle my student in the yoga mat (picture above). She absolutely loves it, and what is more she is calm and steady when usually this child likes to be on the move constantly. Here we have a wonderful moment of joint engagement. She looks at me, she can listen to what I say or sing, and she can tell me in her own way to carry on rolling her or to carry on singing or providing calming pressure to her legs and arms or to stop.
A few pointers for when you try this at home: How to practise containment safely and effectively
Create a safe environment: Ensure the wrapping material is soft, breathable, and free from any hazards.
Observe your child’s cues: Pay attention to your child’s body language and verbal cues to determine their comfort level.
Respect your child’s boundaries: If your child shows signs of distress, stop the containment immediately – this might seem obvious but sometimes we adults get so carried away with some ‘great idea’ that we have seen work elsewhere. And so we can be a little too ‘determined’ sometimes to ‘make it happen’… perhaps this rings a bell with some of my readers.
MAKE IT FUN: Start carefully and take it step by step. See if the student is having a nice time. It is all about trust and therefore it might not work the very first time you do it.
It’s important to remember that containment is not a one-size-fits-all approach. Some children may respond better to other sensory-based interventions. However, for many autistic children containment can be a valuable tool in their journey towards improved communication and emotional regulation.
Feeding and Dysphagia (Swallowing) Specialist The London Speech and Feeding Practice
The London Speech and Feeding Practice
Find a speech and language therapist for your child in London. Are you concerned about your child’s speech, feeding or communication skills and don’t know where to turn? Please contact me and we can discuss how I can help you or visit my services page.