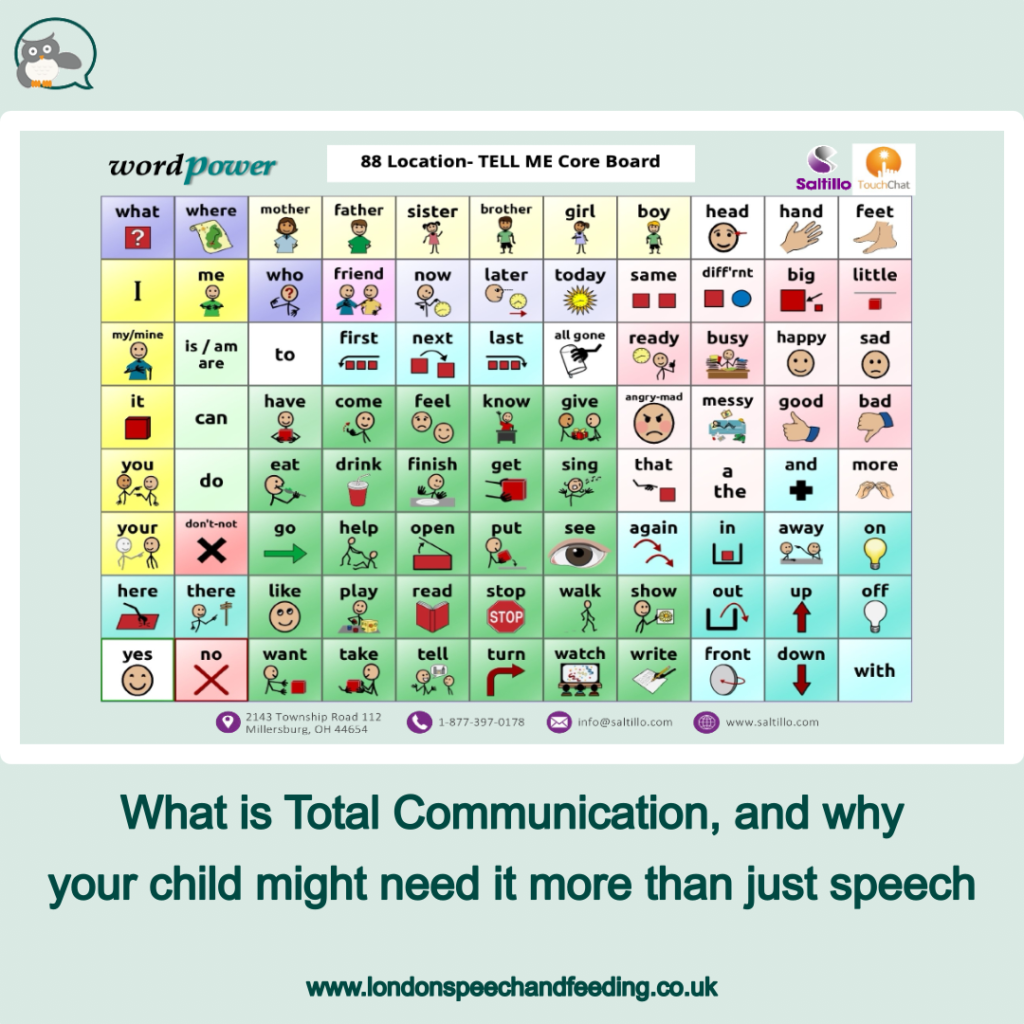
What is Total Communication, and why your child might need it more than just speech

When a child’s speech is difficult to understand, it can feel overwhelming for everyone involved. As a parent, your instinct is often to focus on helping your child ‘talk properly’. And that makes complete sense. Speech is important. But here’s the key message I want to share with you:
Speech is just one way to communicate.
And when speech is not yet clear, not yet reliable, or not yet available, children need other ways to get their message across.
This is where Total Communication comes in.
What is Total Communication?
Total Communication is an approach that encourages the use of all available ways to communicate, not just speech.
This can include:
- spoken words
- gestures and pointing
- facial expressions
- signing (such as Makaton)
- pictures or symbols
- drawing
- electronic AAC (Augmentative and Alternative Communication), such as apps like LAMP Words for Life
It’s not about replacing speech. It’s about supporting communication in every possible way.
Think of it like this: if speech is currently unclear or limited, why restrict a child to the hardest route? Why not give them more tools to succeed?
‘But won’t this stop my child from talking?’
This is one of the most common concerns I hear in clinic.
Parents often worry that if a child starts using signs or a communication device, they will become ‘dependent’ on it and stop trying to talk.
The research tells us something very different.
Studies consistently show that AAC does not prevent speech development. In fact, it often supports it.
- A review by Millar, Light & Schlosser (2006) found that AAC interventions do not reduce speech production and may actually increase it.
- Romski & Sevcik (2005) demonstrated that children given AAC often develop stronger overall communication skills, including spoken language.
- More recent work continues to show that providing AAC early can accelerate language development, not delay it.
So rather than ‘giving up on speech’, using AAC is actually building the foundations that speech needs.
Why Total Communication matters, especially for unintelligible children
When a child is very difficult to understand, they are often experiencing a hidden frustration:
‘I know what I want to say, but no one understands me.’
Over time, this can lead to:
- reduced confidence
- behavioural frustration
- withdrawal from communication
- fewer opportunities to practise language
If a child cannot successfully communicate, they communicate less. And when they communicate less, their language development slows down.
Total Communication breaks this cycle.
By giving a child reliable ways to be understood, we:
- reduce frustration
- increase interaction
- build confidence
- create more opportunities for language learning
And importantly, we allow them to show us what they already know.
AAC is a bridge, not a barrier
Using AAC (whether that’s pointing to pictures, signing, or using a device) does something powerful:
It separates language from speech.
A child might have lots of ideas, vocabulary, and understanding but their speech system (especially in cases like phonological disorder or childhood apraxia of speech) cannot yet keep up.
AAC allows the child to:
- express complex ideas now
- practise sentence structure
- develop vocabulary
- take part in conversations
All while their speech is still developing.
In other words, AAC doesn’t replace speech. It keeps language moving forward while speech catches up.
What does this look like in real life?
In therapy, I often use a combination of approaches:
- modelling simple signs alongside speech
- pointing to symbols while talking
- encouraging children to gesture or show
- using drawings to support understanding
- incorporating an AAC device such as LAMP Words for Life
You might see a child:
- say part of a word
- point to a symbol
- use a gesture
- and look at you expectantly
That is communication success.
And success builds motivation.
‘I just want them to talk’
Of course you do. And I do too!! That’s always the goal.
But here’s the important shift in thinking:
Children learn to talk by communicating, not by waiting until speech is perfect.
If we hold out for clear speech before allowing other communication methods, we risk:
- limiting their ability to interact
- reducing practice opportunities
- increasing frustration
But if we support all communication, we give them:
- more chances to express themselves
- more positive communication experiences
- more input and feedback
And that is what drives progress.
A balanced approach
Total Communication doesn’t mean ‘speech is no longer important’.
It means:
- we continue targeted speech therapy
- we work on sounds and clarity
- and we support communication in the meantime
It’s not either/or.
It’s both/and.
Final thought
If your child’s speech is difficult to understand, the most important question is not:
‘Are they talking clearly yet?’
It’s:
‘Can they successfully communicate?’
Because communication is the foundation of:
- relationships
- learning
- confidence
- wellbeing
And every child deserves a voice, in whatever form that voice takes right now.
Feel free to contact me if your child needs help with speech and communication.

Sonja McGeachie
Highly Specialist Speech and Language Therapist
Owner of The London Speech and Feeding Practice.
References (parent-friendly):
- Romski M & Sevcik R. (2005) Augmentative communication and early intervention: Myths and realities. Infants & Young Children. 18:174-185.
- Millar DC, Light JC, Schlosser RW. (2006) The impact of augmentative and alternative communication intervention on the speech production of individuals with developmental disabilities: a research review. J Speech Lang Hear Res. 49(2):248-264.



Find a speech and language therapist for your child in London. Are you concerned about your child’s speech, feeding or communication skills and don’t know where to turn? Please contact me and we can discuss how I can help you or visit my services page.